Department of Cardiology, University Hospital Ibn Rochd, University Hassan II, Casablanca, Morocco.
Mehdi Belhakim
Email: mbelhakim10@gmail.com
Received : Dec 02, 2024 Accepted : Jan 13, 2025 Published : Jan 20, 2025 Archived : www.meddiscoveries.org
Background: Patent Ductus Arteriosus (PDA) is a congenital heart defect that, if left untreated, can lead to serious complications, including infective endocarditis. Although infective endocarditis primarily affects the left side of the heart, cases involving the right side, particularly the pulmonary valve, are exceedingly rare. Prompt diagnosis and appropriate management are critical to prevent life-threatening outcomes. This case report highlights a rare presentation of pulmonary valve infective endocarditis complicating a PDA, managed surgically with a favorable outcome.
Case presentation: We report the case of a 24-year-old Moroccan woman with no known medical history, who presented with a prolonged febrile illness, dry cough, and exertional dyspnea. Clinical examination revealed fever (38.7°C), tachycardia (112 bpm), and a continuous murmur at the left subclavicular region. Laboratory results indicated a significant inflammatory syndrome with elevated CRP (85 mg/L) and leukocytosis. Echocardiography revealed a 6 mm PDA with vegetations on the pulmonary valve and severe pulmonary insufficiency. Despite an initial response to intravenous antibiotics (gentamycin and ceftriaxone), the patient experienced a recurrence of infective endocarditis, necessitating surgical intervention. She underwent pulmonary valve replacement, mitral vegetectomy, and PDA closure. Postoperatively, the patient’s condition improved significantly, with complete resolution of the infection and restoration of cardiac function.
Conclusion: This case emphasizes the importance of early recognition and aggressive management of infective endocarditis in patients with congenital heart defects such as PDA. Surgical treatment may be necessary in cases where medical management fails. The case also raises the question of whether all PDAs, even small and asymptomatic ones, should be considered for closure to prevent the risk of endocarditis.
Keywords: Patent ductus arteriosus; Infective endocarditis; Pulmonary valve; Cardiology; Cardiac surgery; Morocco.
Infective endocarditis on the right heart is a rare but serious complication of a persistent Patent Ductus Arteriosus (PDA). While antibiotic therapy is typically effective, surgery may be required if the infection cannot be controlled. Without intervention, vegetations may continue to grow, leading to embolization into the lungs or systemic circulation [1,2].
We report the case of a 24-year-old woman with pulmonary valve infective endocarditis associated with a PDA, successfully treated via Cardiopulmonary Bypass (CPB), with favorable postoperative outcomes.
Ms. E.Z, a 24-year-old female with no known medical history, was admitted to the cardiology department at Ibn Rochd University Hospital with symptoms of prolonged fever, dry cough, and exertional dyspnea that had persisted for two weeks prior to admission, in the context of general health deterioration. Clinical examination revealed a febrile patient with a temperature of 38.7°C, tachycardia at 112 bpm, normal blood pressure (130/80 mmHg), and resting eupnea. A continuous murmur was heard under the left clavicle, grade 2/6, and a vascular purpura localized to the lower extremities was noted on skin examination. Oral examination revealed poor dental hygiene. No other significant findings were noted on systemic examination.
The Electrocardiogram (ECG) showed sinus tachycardia at 110 bpm with no other abnormalities. Laboratory findings supported an inflammatory syndrome with hypochromic microcytic anemia (hemoglobin: 10 g/dl), leukocytosis (white blood cell count: 13,000, predominantly neutrophils), and an elevated C-reactive protein (CRP) at 85 mg/dl. Electrolyte levels, renal function, and liver function were within normal limits. Platelet count was normal (208,000), and rheumatoid factor was positive. Blood cultures were negative, and other lab tests showed no significant abnormalities.
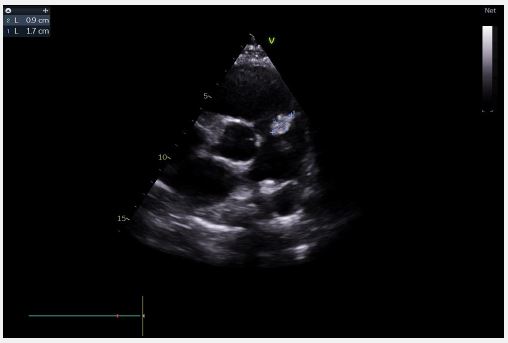
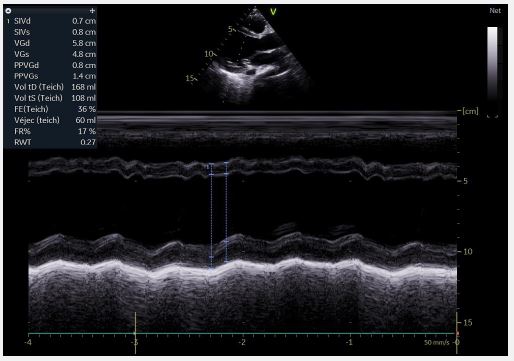
Echocardiography revealed a restrictive PDA with a 6-mm diameter and a significant gradient, along with mobile vegetation attached to the pulmonary valve leaflets and the origin of the pulmonary artery (Figure 1), leading to severe pulmonary insufficiency. The mitral valve was calcified with a vegetation measuring 11×7 mm, and mild mitral regurgitation was noted. The Left Ventricle (LV) was dilated with reduced ejection fraction (Figure 2). The Right Ventricle (RV) was non-dilated with preserved systolic function. The Inferior Vena Cava (IVC) was slightly dilated but compliant. Extension investigations found no septic emboli.
A parenteral antibiotic regimen, consisting of gentamicin (5 mg/kg/day for 15 days) and ceftriaxone (2 g/day for 4 weeks), was initiated, along with furosemide 40 mg/day and dental care. Clinical, biological, and echocardiographic improvements were observed. However, one month later, the patient returned with a recurrence of infective endocarditis, presenting with right heart failure, necessitating surgical intervention.
The surgical approach involved the implantation of a mechanical pulmonary valve prosthesis, mitral vegetation removal, and PDA closure using a patch. The postoperative course was favorable, with the patient becoming afebrile after seven days. Echocardiographic follow-up showed a well-functioning pulmonary valve prosthesis, no mitral vegetations, good LV function, and significant improvement in RV function. The patient was discharged after 10 days on acenocoumarol 4 mg (1 tablet/day), bisoprolol 2.5 mg/day, and furosemide 40 mg/day.
Before the advent of antibiotics, infective endocarditis was a severe complication of PDA, associated with high morbidity and mortality [3,4]. With the development of therapeutic options, cases of infective endocarditis in PDA patients have become exceedingly rare [1,5]. Although PDA remains a risk factor for infective endocarditis, particularly in developing countries, antibiotic prophylaxis is not routinely recommended [6].
Several case reports have shown that the size of the ductus arteriosus does not necessarily correlate with the risk of developing infective endocarditis [7,8]. Instead, the hemodynamic turbulence between the aorta and pulmonary artery, which leads to endothelial injury and subsequent pathogen deposition on the damaged endothelium, is considered the key mechanism driving vegetation formation, particularly in patients with PDA [9].
Thus, the prophylactic closure of small, restrictive, and asymptomatic PDAs could be considered a preventive measure, although there are no strong recommendations supporting the closure of asymptomatic small PDAs [10,11].
In this case, surgical intervention was indicated due to the recurrence of infective endocarditis and the worsening clinical symptoms, particularly the onset of right heart failure. This observation supports the hypothesis that even small PDAs should be systematically closed to prevent the development of infective endocarditis.
Infective endocarditis is a rare but severe complication of PDA. Advances in therapeutic options have significantly reduced morbidity and mortality in this population. Through this clinical case, we highlight the importance of maintaining good oral hygiene, early diagnosis, and appropriate management of PDAs to prevent severe complications.
Teaching points
• Infective endocarditis involving the pulmonary valve is rare and may complicate even small PDAs.
• Early surgical intervention is crucial in cases of recurrent endocarditis to prevent irreversible damage.
• This case underscores the potential need for prophylactic closure of asymptomatic PDA to prevent infective endocarditis.
Abbreviations: PCA: Patent Ductus Arteriosus; IE: Infective Endocarditis; TTE: Transthoracic Echocardiography; CRP: C-Reactive Protein; PCR: Polymerase Chain Reaction; Vmax: peak tricuspid regurgitation velocity; PAH: Pulmonary Arterial Hypertension; PH: Pulmonary Hypertension.
Ethics approval and consent to participate: This case report was conducted in accordance with the declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a health insurance portability and accountability Act. we know of no conflicts of interest associated with this publication.
Consent for publication: Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials: The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding: There has been no significant financial support for this work that could have influenced its outcome.
Author’s contributions: MB, AA, and SE designed the research. HR, AD, and contributed to the bibliographical research. AB contributed to the figures’ formation. MB wrote the article.
Acknowledgements: We thank all staff of UHC Ibn Rochd who contributed to this report.
