1Department of Pharmacy, Guangxi Academy of Medical Sciences and the People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning 530021, China.
2Department of Emergency, The Third Affiliated Hospital of Guangxi Medical University, Nanning 530031, China.
#These authors have been equally contributed to this article.
Xiaoyu Chen
Email: chenxiaoyu166@outlook.com & 254930320@qq.com
Received : Dec 05, 2024 Accepted : Jan 10, 2025 Published : Jan 17, 2025 Archived : www.meddiscoveries.org
Early nutritional intervention is a crucial consideration in the management of acute pancreatitis, as the presence of nutritional risk can significantly impact the prognosis of the condition. This meta-analysis aims to investigate the effects of early enteral nutrition on patients with acute pancreatitis, assessing both the safety and efficacy of this therapeutic approach.
We searching major databases including China Knowledge, Wanfang Database, PubMed, Cochrane Library and Embase. In this study, we applied the Cochrane Rob2 scale to thoroughly assess the risk of bias of individual studies. These assessments helped us to ensure that our analyses were based on a solid research foundation. We conducted Meta-analyses using Stata 17.0 software to synthesise the results of the studies. We also used the I2 test to assess the heterogeneity among the studies. This step helped us to reveal the differences between studies to better understand the effect of nutritional support on patients with acute pancreatitis. In conclusion, early enteral nutritional intervention can improve mortality, complication, intolerance of feeding in patients with AP, reduce the length of hospital stay, and are pronounced in patients with moderate to severe pancreatitis.
Acute Pancreatitis (AP) is an inflammatory disease of the pancreas caused by the self-cancellation of the pancreas. The pathophysiology of this disease occurs when the normally inactive protease precursors secreted by the alveolar cells are prematurely activated and as a result produce auto digestion [1]. Overall, it has a global incidence of 30-40 cases per 100,000 population per year, a small number (about 15%-20%) may be associated with persistent organ failure and develop to Severe Acute Pancreatitis (SAP) [2]. The mortality rate of SAP is significantly higher than that of AP, and once the infection is secondary, the average mortality rate increases to about 30% [3]. In traditional treatment, in order to avoid the Pancreatic fluid secretion stimulation caused by the pain and pancreatitis aggravation [4], advocate fasting to let the pancreas get adequate rest as the basic treatment for AP [5,6]. A number of studies have questioned the validity of early fasting to give the pancreas a rest [7,8]. Besides, fasting may lead to intestinal mucosal atrophy, epithelial barrier dysfunction, and the intestine the change in the microflora, especially in some AP patients, may even be initiated Sepsis and organ failure [9-11].
In recent years, Early Enteral Nutrition (EEN) has garnered significant attention in the management of patients with Severe Acute Pancreatitis (SAP). EEN not only preserves the homeostasis of the intestinal flora and the integrity of the intestinal mucosa but also promotes the repair of damaged intestines and diminishes intestinal injury [12,13]. A recent meta-analysis evaluating five studies showed that compared with early refeeding, immediate EEN after admission could safely reduce LOHS and intolerance of feeding in patients with AP [14]. This result is consistent with another study evaluating 11 randomized trials, which showed that EEN significantly reduced the risk of mortality, infection and complications in SAP patients, EEN support also reduced the incidence of MOF and surgical interventions [15]. Therefore, the American Gastroenterological Association and the European Society for Parenteral and Enteral Nutrition recommend that patients with SAP and patients with mild to moderate AP who are unable to consume food by mouth should be given priority to EEN [16,17]. However, some studies point to controversial areas where EEN, while accelerating recovery, increases adverse gastrointestinal events [18-20]. Therefore, we conducted a systematic review and meta-analysis in order to assess the efficacy and feasibility of EEN in patients with AP. We also attempted to determine the optimal timing for early onset of EEN.
Protocol and registration
In addition to the PRISMA guidelines, we followed the Cochrane Handbook for Systematic Reviews of Intervention [21]. The protocol for this systematic review and meta-analysis was registered in PROSPERO (no. CRD42023429352).
Search strategy
We performed a literature search in various databases such as China National Knowledge Infrastructure, Wanfang Database, China Science and Technology (Sci-Tech) Journal Database, PubMed, Cochrane Library, Embase, and Web of Science databases. The keywords used for the search included “acute pancreatitis, nutrition, enteral nutrition,” “randomized controlled trial, and controlled clinical trial.” Literature searches were conducted using medical subject headings (MeSH) and synonyms. The detailed search strategy is available in Supplementary Table S1. The search period spanned from inception to May 2024.
Study eligibility criteria
The study type should have been an RCT on nutritional support.
The study population should have included acute pancreatitis, both mild and severe are accompany.
The interventions in the experimental group should have been clearly described.
The study should have passed ethical review.
Primary outcomes: Relevant nutritional indicators reported in the literature, such as, mortality, organ failure, hospitalization time, pancreatic necrosis, Systemic Inflammatory Response Syndrome (SIRS).
Secondary outcomes: Infection.
Exclusion criteria
Duplication of the same literature in different databases.
Study population concurrently experienced other cancers.
Receipt of other drugs or treatments that may affect the observed nutritional indicators.
Literature with flaws in study design.
Literature for which complete data are not available or full text is not available.
Literature other than RCTs.
Selection of studies and data extraction
Literature search of the databases was conducted by two researchers (Tan and He), wherein they performed an initial screening of the titles and abstracts and removed duplicates to ensure that each article was screened and evaluated, and in case of disagreement between the two reviewers, a third researcher made the assessment. One researcher (Li) extracted data from the retrieved literature, including information on primary and secondary outcome indicators. Then two researchers (He and Chen) cross-reviewed and collated the tables. They ensured that basic information about the article, such as literature title, authors details, year of publication, study population, intervention, and conclusion, was collected.
Risk of bias assessment
The methodological quality of the included randomized controlled trials (RCTs) was evaluated by two independent researchers, He and Qin, employing the criteria outlined by the Cochrane Literature Quality Assessment Tool. This evaluation encompassed seven key domains: 1) the method for generating the random allocation sequence, 2) allocation concealment, 3) blinding of investigators and participants, 4) blinding of outcome assessors, 5) the completeness of outcome data, 6) selective reporting of study findings, and 7) any other potential biases. These domains were utilized to categorize the articles into three risk levels: “low risk,” “some concerns,” and “high risk” [22].
Data analysis
The meta-analysis was performed using STATA 17.0. Systematic evaluation was performed through a meta-analysis of mortality, organ failure, Hospitalization time, Pancreatic necrosis, SIRS, CRP. Data were analyzed using the STATA 17.0 statistical package (Cochrane Collaboration Software). Data of dichotomous outcomes were expressed as odds ratios with 95% Confidence Intervals (CIs) and Standardized Mean Difference (SMD). A test of heterogeneity was performed with the I2 test and Q statistic. An I2 value of >50% or P value of < 0.05 was assumed to indicate significant heterogeneity. Publication/reporting biases were visually assessed using funnel plots. If there was no observed heterogeneity, then the fixed-effects model was chosen; otherwise, the random-effects model was used [23,24].
Study identification and selection
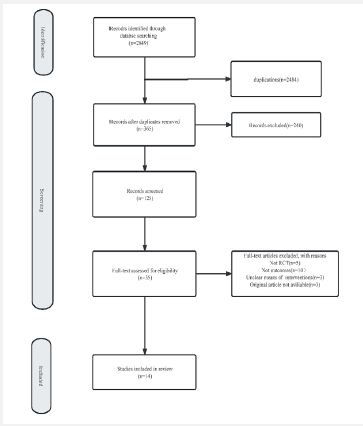
The search strategy yielded a total of 2849 records, 365 records remaining after initial screened wherein 240 duplicate studies were removed, remained after initial screening and re-screening according to the inclusion and exclusion criteria, the remaining literature was re-evaluated to exclude articles that were not RCTs, those for which the original text was not available, those that did not describe outcome indicators, and those that had evaluated nonprime lesions; altogether, only 14 studies (nine in English and five in Chinese) were included for analysis (Figure 1). The total sample size of the included studies was 1381 patients. Details of the 14 RCTs [25-38] included in the meta-analysis are listed in Table 1.
| Author | Year | Country | ENstarted within admission | Severity of AP | Sample size | Outcomes | |
|---|---|---|---|---|---|---|---|
| Experiment | Control | ||||||
| Olah | 2002 | Hungary | <24 h after admission | AP | 41 | 48 | ①②④ |
| Eckerwall | 2006 | Sweden | <24 h after admission | SAP | 24 | 26 | ①②③④⑥ |
| Petrov | 2007 | Russia | <24 h after admission | SAP | 35 | 34 | ①②④⑥ |
| Casas | 2007 | Spanish | <24 h after admission | SAP | 11 | 11 | ④⑤ |
| Wereszczynska | 2013 | Poland | <48 h after admission | AP | 97 | 100 | ①②③④⑤⑥ |
| SUN | 2013 | China | <48 h after admission | SAP | 30 | 30 | ①②⑤⑥ |
| Bakker | 2014 | Holland | <24 h after admission | AP | 101 | 104 | ①②④⑤ |
| Stimaca | 2016 | Croatia | <24 h after admission | AP | 107 | 107 | ①②③④⑤ |
| XU | 2018 | China | <24 h after admission | SAP | 26 | 29 | ①②③④⑤ |
| BI | 2020 | China | <48 h after admission | SAP | 53 | 50 | ①②③⑤⑥ |
| Esmer | 2021 | Mexico | <24 h after admission | AP | 29 | 30 | ⑥ |
| Cao | 2021 | China | <72h afteradmission | SAP | 42 | 40 | ②③④⑥ |
| Fang | 2022 | China | <24 h after admission | SAP | 30 | 30 | ①②⑥ |
| Feng | 2023 | China | <24 h after admission | SAP | 58 | 58 | ①②③⑥ |
| ①mortality ②Multiple organ failure ③hospitalization time ④Pancreatic necrosis ⑤SIRS ⑥CRP | |||||||
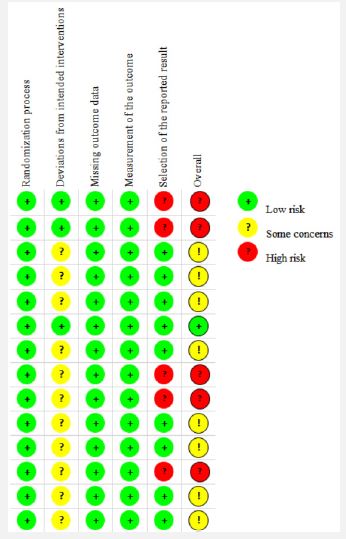
The risk of bias of the included studies was evaluated by two researchers (He and Tan), using the risk of bias tool ROB2.0 of the Cochrane Handbook for Systematic Evaluation of Interventions [22]. The risk of bias was calculated by evaluating the following areas of bias: randomization process, deviation from established interventions, missing outcome data, outcome measures, selective reporting of outcomes, and overall bias assessment. Only one study had a low risk of bias [30], while almost half of the RCTs had some risk of bias owing to unclear allocation sequence concealment methods or the influence of the study setting [27-29,31,34,35,37,38], and five studies had a high risk of bias owing to problems with outcome measures [25,26,32,33,36]. The results of the risk of bias assessment are presented in Figure 2.
Mortality
Eleven studies (1381 patients) analyzed the mortality of AP with nutritional support. EEN compared with late EN or TPN, the meta-analysis indicated that there was significant difference in the value of change in mortality (RR=0.60, 95% CI: 0.40 to 0.90, P=0.014; Figure 3), as determined using a random-effects model and that there was heterogeneity between studies (I2=25.7%, P=0.47).
Length of hospital stay
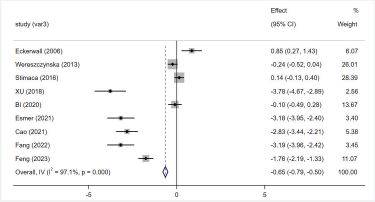
The nine included studies reported LOHS involving 970 patients offered the specific data. The meta-analysis suggested that EEN could significantly decrease the LOHS, compared with late EN or TPN (SMD=-1.16, 95% CI: -2.41 to -0.63; P=0.001, I2=97.1%; presented as Figure 4).
Organ failure
There were eleven studies providing the specific information about progression to acute pancreatitis, the meta-analysis involving 1240 patients revealed that EEN significantly increase the number of progressions to severe pancreatitis compared with late EN or TPN (RR=0.58; 95% CI: 0.44 to 0.76; P=0.000, I2=1.8%; Figure 5).

Pancreatic necrosis
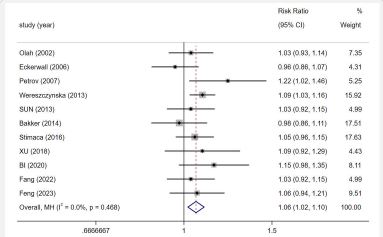
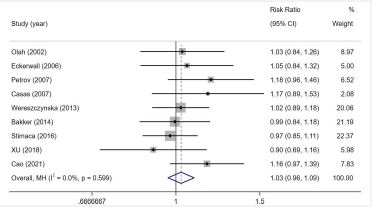
Among the included studies, nine described pancreatic necrosis, no significant difference was observed in the change in pancreatic necrosis in AP of accepting the EEN and control groups (RR=0.92, 95% CI: 0.75 to 1.14, P>0.05, I2=24.0%; Figure 6).
SIRS
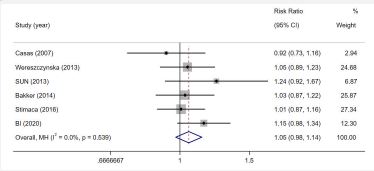
Only six studies involving 801 patients reported the patients’ systemic inflammatory response syndrome. The pooled result of the six studies showed EEN had no significant decrease compared with late EN or TPN (RR=0.83; 95% CI: 0.68 to 1.02; P>0.05, I2=36.5%; presented as Figure 7).
Infection
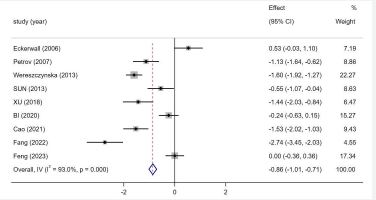
C-reactive protein: The nine included studies reported CRP involving 792 patients offered the specific data. The meta-analysis suggested EEN could significantly decrease the level of CRP, compared with late EN or TPN (SMD =-0.95; 95% CI: -1.54 to -0.36; P=0.002, I2=93.0%; presented as Figure 8).
Pancreatic infection complications
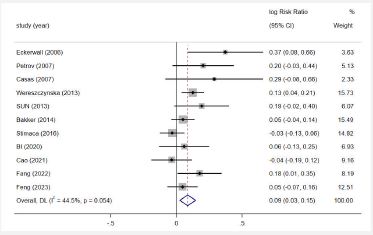
Eleven studies reporting the incidence of pancreatic infection complications of AP were pooled. A significant reduction was detected when comparing EEN with late EN or TPN (RR=0.52; 95% CI: 0.35 to 0.79, P=0.002, I2=50.9%; Figure 9).
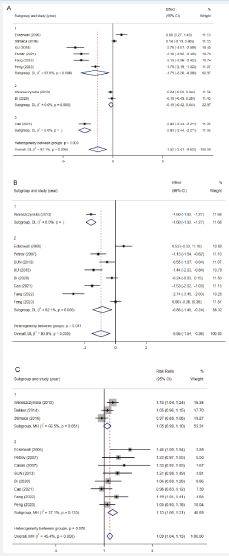
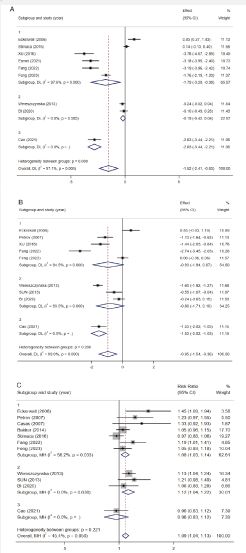
Subgroup analysis of LOHS and infection
The test for heterogeneity in this study was significant, indicating heterogeneity between the included studies outcomes. To analyze the sources of heterogeneity, subgroup analyses were conducted according to the Atlanta Classification of pancreatitis patients and time of enteral nutrition intervention.
All of the studies were grouped according to the Atlanta Classification of patients: AP and SAP. Subgroup analysis indicated that EEN of AP could decrease the CRP and EEN of SAP could decrease the LOHS, CRP and PIC. Another group approach was based on the time of EN: <24h, <48h, <72h. The results showed that early 24h EN could decrease the LOHS and PIC, early 48h EN could decrease the PIC and early 72h EN could decrease the LOHS and CRP (Table 2, Figures 10, 11).
| LOHS | Infection | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CRP | PIC | |||||||||||
| Subgroups | Trials | RR/SMD | I2 | P | Trials | RR/SMD | I2 | P | Trials | RR/SMD | I2 | P |
| Subgroups analysis via Atlanta Classification | ||||||||||||
| AP | 3 | -1.008 | 96.80% | 0.092 | 1 | -1.596 | NA | 0.000 | 3 | 1.046 | 66.50% | 0.089 |
| SAP | 6 | -1.775 | 97.10% | 0.009 | 8 | -0.863 | 92.10% | 0.007 | 8 | 1.131 | 37.10% | 0.000 |
| Subgroups analysis via time of enteral nutrition intervention | ||||||||||||
| <24H | 6 | -1.789 | 97.60% | 0.013 | 5 | -0.934 | 94.50% | 0.068 | 7 | 1.081 | 56.20% | 0.004 |
| <48H | 2 | -0.19 | 0.00% | 0.100 | 3 | -0.804 | 93.50% | 0.082 | 3 | 1.124 | 0.00% | 0.004 |
| <72H | 1 | -2.827 | NA | 0.000 | 1 | -1.528 | NA | 0.000 | 1 | 0.964 | NA | 0.644 |
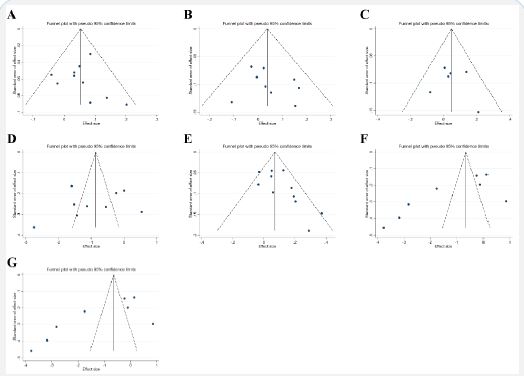
Publication bias analysis
As displayed in the funnel plots of mortality, pancreatic necrosis, SIRS, and infection, the symmetrical figures indicated that there was no publication bias (Figure 12), and the results showed an asymmetric LOHS funnel plot with Egger’s test P=0.015, an asymmetric organ failure funnel plot with Egger’s test P=0.004, indicating a possible risk of publication bias (Figure 12). Furthermore, the cut-and-patch method was performed, and the results were stable before and after the cut-and-patch method; publication bias had only less effect on the authenticity of the results.
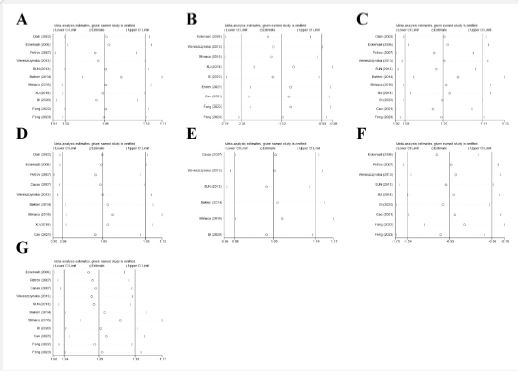
Sensitivity analyses
Sensitivity analyses were conducted using the study-by-study approach. The results showed no significant change in the heterogeneity between studies, indicating a degree of reliability, possibly suggesting that the influencing factors in this meta-analysis are stable (Figure 13).
Discussion/conclusion
Nutritional support plays an important role in the management of patients with pancreatitis [39]. The European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines recommend that for patients with acute pancreatitis, early oral feeding or enteral nutrition is recommended as tolerated, rather than fasting the patients. This is because early feeding has been shown to reduce the risk of infectious complications and shorten hospital length of stay, without increasing the risk of adverse events. However, the timing and type of feeding should be individualized based on the severity of the disease, presence of complications, and patient tolerance. It is important for patients with acute pancreatitis to be closely monitored by their healthcare provider and registered dietitian to ensure that their nutritional needs are met while minimizing the risk of complications [16]. In recent years, several studies have explored when to enable EN [40-42], and there is still a lack of a strong evidence-based basis. Hence, there is currently a clinical debate about the timing of early implementation of EN.
The study has assessed the effectiveness and safety of EEN by examining outcomes including the duration of length of hospital stay, the incidence of infectious complications, and indicators of inflammation. The findings may contribute to the development of clinical practice guidelines for the treatment of AP and the implementation of nutritional support. Upon meta-analysis of the data, it was determined that administering EEN post-admission not only decreases mortality rates but also leads to a reduced hospital stay. Furthermore, EEN was found to diminish the occurrence of organ failure and infections in comparison to delayed EN or TPN. Nevertheless, no significant variance was noted in the rates of pancreatic necrosis and Systemic Inflammatory Response Syndrome (SIRS).
In this study, subgroup analysis was performed for the LOHS and Infections, which are the most heterogeneous of the outcome indicators, and the results showed that EN had a statistically significant effect on the LOHS and Infections in SAP. Another set of results showed that EN reduced LOHS and infections except for < 24H which was ineffective for CRP and <48H which was ineffective for LOHS and CRP. We therefore suspect that the time of administration of EN is one of the sources of heterogeneity.
As shown by the funnel plot, there may have been some publication bias in LOHS and organ failure, which may be due to the small number of English-language publications included in the meta-analysis; articles with positive results, compared with negative results, being more likely to be published; and the fact that some RCTs did not have detailed data.
Several limitations of this study include the small sample size and the average quality of the literature, thus limiting the generalizability of the results obtained from this study; the difficulty of allocation concealment and blinded implementation attributed to the methodology of nutritional support for clinical events; the lack of specific data on other indicators such as liver and renal function (bilirubin and transaminases) and prognostic nutritional indices, which did not allow for systematic analysis; and the number of certain indicators included in the literature The heterogeneity among studies may be influenced by factors such as the hospitality and recovery of the gastrointestinal tract function. Therefore, there is an urgent need for more clinical RCTs with large sample sizes, multiple assessment indicators, and long intervention and follow-up durations to assess the effectiveness of nutrition studies in patients with pancreatitis. This study is referring to aimed to update and expand upon a previously published meta-analysis on the use of EEN in patients with pancreatitis. By including updated RCTs and performing two subgroup analyses, subgroup analyses can be useful in identifying specific patient populations that may benefit more from a particular intervention. By conducting subgroup analyses based on different factors, such as disease severity or etiology, the study may have provided more nuanced and personalized recommendations for the use of EEN in patients with pancreatitis. the study aimed to provide more objective and comprehensive conclusions regarding the efficacy and safety of EEN in this patient population.
Mette argued as early as 1997 that critically ill patients can be saved with EEN support [43]. Guidelines in many countries recommend that patients with pancreatitis should start EN this morning [16,44]. In many countries, the concept of early EEN is commonly used in clinical practice, but it is controversial, mainly because there is no consensus on the timing of EEN. A retrospective study evaluating the impact of Parenteral Nutrition (PN) versus oral/Enteral Nutrition (EN) on clinical and economic outcomes in AP, enrolling 171 patients, resulted in a reduction in LOHS and total hospitalization costs in the PN versus EN group [45]. A meta-analysis shows EN is more effective and safer compared to late enteral nutrition [46]. This result is consistent with another meta-analysis of EEN provided within 24 hours of admission on clinical outcomes in AP, mortality and multi-organ failure outcomes in EEN are superior to parenteral or delayed enteral nutrition [47]. Most studies have defined EEN as occurring within 24 to 48H, these studies suggest that patients with AP have significantly increased intestinal permeability after 72H or more, and that the inflammatory response causes more damage [48,49]. Therefore, our findings suggest that early 24H enteral nutrition is more conducive to the clinical outcome of patients with pancreatitis, and severity of AP patients should be assessed as early as possible and nutritional intervention should be provided.
This meta-analysis found that EN can improve nutrition for pancreatitis patients, especially moderate to severe cases, contributing to better clinical outcomes. However, larger multi-center studies with stricter methods are needed to strengthen the evidence before making clinical decisions due to limitations.
Ethics approval: Ethics approval was not required as this study relied on published and publicly available data.
Data availability statement: Data availability is not applicable to this article as no new data were created or analyzed in this study.
