1Henan High-Tech Industrial Company Limited, Henan Academy of Sciences, Zhengzhou 450002, China.
2Department of Orthopedics, Zhengzhou University People’s Hospital, Henan Provincial People’s Hospital, Zhengzhou 450003, China.
#These authors have been equally contributed to this article.
Hongjun Zhang
Email: zdzhj20001@163.co
Received : Dec 04, 2024 Accepted : Jan 07, 2025 Published : Jan 14, 2025 Archived : www.meddiscoveries.org
Objective: This study aims to compare the short- and long-term effects of intra-articular Platelet-Rich Plasma (PRP) injections combined with acupoint injections versus PRP injections alone and Hyaluronic Acid (HA) intra-articular injections in the treatment of knee osteoarthritis.
Methods: Ninety patients with knee osteoarthritis were randomly divided into three groups: (1) PRP combined with acupoint injection (30 patients); (2) PRP intra-articular injection alone (30 patients); and (3) HA intra-articular injection alone (30 patients). Outcomes were assessed using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Hospital for Special Surgery (HSS) score, Knee Society Score (KSS), and Visual Analogue Scale (VAS) to evaluate pain, mobility, activity level, joint stability, daily life impact, and patient satisfaction. Independent evaluators conducted all scoring and statistical analyses.
Results: The cohort had a mean age of 52.3 ± 0.96 years and consisted of 55.7% females and 44.3% males. All groups showed significant improvements in knee pain, mobility, and satisfaction within 1 to 3 months post-injection compared to baseline, with the HA group demonstrating the most pronounced short-term benefits (P< 0.05). At the 6-month follow-up, the PRP combined with acupoint injection group and PRP injection group exhibited superior outcomes compared to the HA group (P<0.05). By 12 months, the PRP combined with acupoint injection group achieved significantly better scores than both the PRP injection and HA groups (P< 0.05).
Conclusion: Combining PRP injections with acupoint injections at Blood Sea, Yanglingquan, and Huizhong points provides significant and sustained improvements in symptom relief and knee joint mobility for patients with knee osteoarthritis.
Keywords: Platelet-rich plasma; Hyaluronic acid; Osteoarthritis of the knee; Acupoint injection
Knee Osteoarthritis (KOA) is the most common joint disease among individuals over the age of 60, causing joint pain, functional limitations, and disability on a global scale. The condition is marked by progressive degeneration of articular cartilage, remodeling of subchondral bone, and synovitis, which collectively lead to structural and functional joint damage [1].
Treatment options for KOA are diverse and can be broadly categorized into surgical and conservative approaches. While surgical interventions can be effective, they are not suitable for all patients and carry risks such as periprosthetic infections, fractures, and prosthetic wear. These complications often necessitate additional surgeries, resulting in significant financial burdens and emotional distress for patients and society alike [2].
Among non-surgical treatments, acupoint injection has attracted increasing attention from clinicians. Studies have demonstrated its efficacy in managing KOA as well as other conditions, including facial neuritis, rheumatoid arthritis, and acute lumbar spine symptoms [3-6]. Similarly, autologous Platelet-Rich Plasma (PRP) therapy has been recognized as a safe and effective non-surgical option for KOA. A wealth of domestic and international research has shown that PRP injections can significantly alleviate pain and slow disease progression in KOA patients.
However, no studies to date have examined the potential benefits of combining intra-articular PRP injections with peripheral acupoint injections for treating KOA. Building upon the existing body of evidence, this study aims to investigate the effects of integrating PRP knee joint cavity injections with peripheral acupoint therapy in managing early-stage KOA.
Patients
The study protocol was approved by the Ethics Committee of Henan Provincial People’s Hospital (No.32,2023), and all patients signed informed consent. This study collected the general data of 90 patients with KOA in outpatients and wards of Henan Provincial People’s Hospital from January 2023 to December 2023, to compare the long-term effects of intra-articular PRP combined with acupoint PRP, intra-articular PRP, and intra-articular HA on symptoms in patients with mild to moderate osteoarthritis. The recruitment criteria were as follows: 1. chronic joint pain or swelling (>4 months); 2. It meets the diagnostic criteria of the Chinese Guidelines for the Diagnosis and Treatment of Osteoarthritis (2021 Edition), and the X-ray evaluation results meet the Kellgren-Lawrence scale (K-L scale) level I to level III [7]. And the exclusion criteria were as follows: 1. age over 80 years old; 2. K-L classification is greater than Ⅲ grade; 3. Combined with rheumatoid arthritis, severe osteoporosis, tumor, gout, obvious joint deformity and other diseases; 4. Poor compliance, not according to the provisions of treatment; 5. Pregnant and lactating women; 6. Patients voluntarily withdrew from the study; 7. Patients were lost to follow-up due to various reasons during follow-up.
Treatment methods
A total of 90 participants were randomly assigned to one of three groups, with 30 patients in each group: HA Group: Patients received intra-articular injections of hyaluronic acid (2 mL per injection) along with simultaneous normal saline injections (1 mL) at the Xuehai, Yanglingquan, and Weizhong acupoints. Treatments were administered once weekly for 4 consecutive weeks.
PRP group: Patients received intra-articular injections of Platelet-Rich Plasma (PRP, 3.5 mL per injection) alongside simultaneous normal saline injections (1 mL) at the Xuehai, Yanglingquan, and Weizhong acupoints. Treatments were administered once weekly for 4 consecutive weeks. PRP + Acupoint Group: Patients received intra-articular injections of platelet-rich plasma (PRP, 3.5 mL per injection) along with simultaneous PRP injections (1 mL) at the Xuehai, Yanglingquan, and Weizhong acupoints. Treatments were administered once weekly for 4 consecutive weeks.
Autologous PRP Preparation
A total of 18 mL of venous blood was collected from the patient’s upper limb and mixed with 2 mL of anticoagulant glucose citrate solution. The sample was subjected to centrifugation in a low-speed centrifuge at 1400 rpm for 10 minutes (Figure 2). Approximately 3 mL of plasma was carefully aspirated from the interface of the red blood cell layer. This plasma was then centrifuged again at 1400 rpm for an additional 10 minutes, allowing the separation of approximately three-quarters of the upper platelet plasma to yield platelet-rich plasma (PRP). The PRP was activated by adding 0.2 mL of calcium chloride. The entire preparation process was conducted under sterile conditions and passed Good Manufacturing Practice (GMP) testing, ensuring the safety of the participants [8].
Observation index and criterion of curative effect
The level of pain relief following treatment was assessed in the three groups using the Visual Analog Scale (VAS), which ranges from 1 to 10, with lower scores indicating less pain intensity. Knee joint function was evaluated using the Knee Society Score (KSS), which includes five major components, totaling a maximum of 200 points. Higher scores reflect better knee joint function. The severity of knee osteoarthritis was measured using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), consisting of 24 items with a maximum score of 240 points, where lower scores indicate less severe osteoarthritis. Treatment efficacy was determined by calculating the total effective rate, defined as the percentage of cases showing significant improvement, effectiveness, or moderate improvement, divided by the total number of cases and multiplied by 100%. The improvement rate was calculated as the difference between WOMAC scores before treatment and at 12 months, divided by the pre-treatment WOMAC score, and then multiplied by 100%. Treatment effectiveness was categorized as follows: Obvious Effect (>70% improvement), Effective (50-70% improvement), Improvement (30-50% improvement), and Ineffective (< 30% improvement).
Statistical analysis
The data from this clinical trial were analyzed using SPSS version 26.0 statistical software. Continuous variables are presented as mean ± standard deviation (x̅ ± s). The independent sample t-test was used to compare continuous data between groups, and the Chi-square test was applied for the analysis of categorical data. Two-factor repeated measures ANOVA was employed to compare WOMAC, AKS, and VAS scores over time. A significance level of P< 0.05 was considered statistically significant.
The baseline characters of cases
The demographic and clinical data comparisons among the three groups are summarized in Table 1 and Table 2. A total of 90 KOA patients were initially enrolled; after accounting for dropout cases, 70 participants completed the study. In the HA group, 30 patients were recruited, with 7 cases lost to follow-up, leaving 23 participants (10 males, 13 females; mean age: 52.74 ± 0.83 years). In the PRP group, 30 patients were recruited, with 9 cases lost to follow-up, leaving 21 participants (9 males, 12 females; mean age: 52.66 ± 1.02 years). In the PRP combined with acupoint injection group, 30 patients were recruited, with 4 cases lost to follow-up, leaving 26 participants (12 males, 14 females; mean age: 51.62 ± 0.96 years). Statistical analysis revealed no significant differences in demographic or baseline clinical characteristics among the three groups (P>0.05), confirming their comparability.
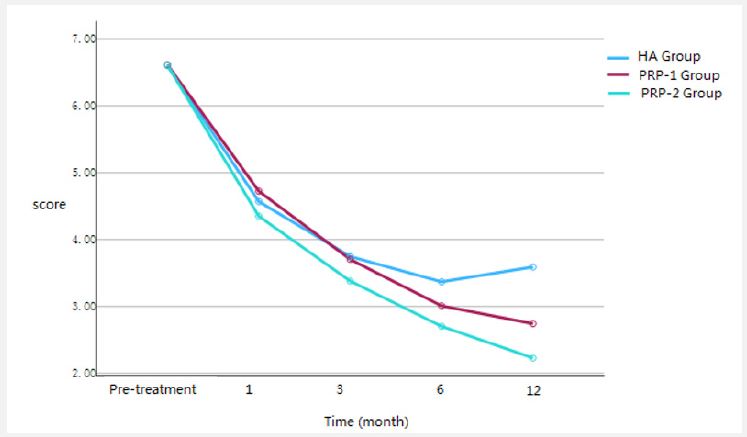
Comparison of VAS pain scores
The VAS pain scores for all three groups are presented in Table 3 and Figure 1. Pain scores were significantly reduced in all groups at 1, 3, and 6 months post-treatment compared to baseline (P< 0.05). At 1 and 3 months post-treatment, there were no statistically significant differences in pain scores among the three groups (P>0.05). By 6 months, the PRP injection group demonstrated significantly lower pain scores than the HA group (P< 0.001). At 12 months post-treatment, the HA group exhibited an increase in pain scores, whereas both the PRP routine injection group and PRP acupoint injection group showed a continued decrease in pain scores. The PRP acupoint injection group demonstrated significantly lower pain scores than both the HA group (P2< 0.001) and the PRP routine injection group (P3=0.001). These findings suggest that while short-term pain relief (< 6 months) did not differ significantly among the three groups, long-term follow-up (>12 months) revealed superior pain relief in the PRP acupoint injection group compared to the HA and PRP routine injection groups.
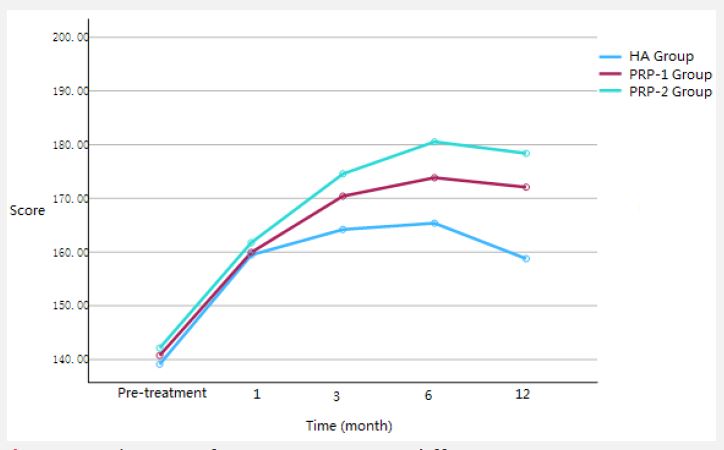
Comparison of KSS joint function scores
KSS joint function scores are presented in Table 4 and Figure 3. At 1 and 3 months post-treatment, all three groups demonstrated significant improvements in joint function compared to baseline (P< 0.05), with no significant differences among the groups. However, at 6 and 12 months, the joint function scores in all groups continued to improve (P< 0.05). The PRP acupoint injection group exhibited significantly higher scores than the PRP routine injection group and the HA group (P2< 0.001, P3< 0.001). These results indicate that while short-term joint function recovery (< 3 months) was similar across the three groups, long-term follow-up (>6 months) highlighted the superior efficacy of the PRP acupoint injection group in restoring joint function.
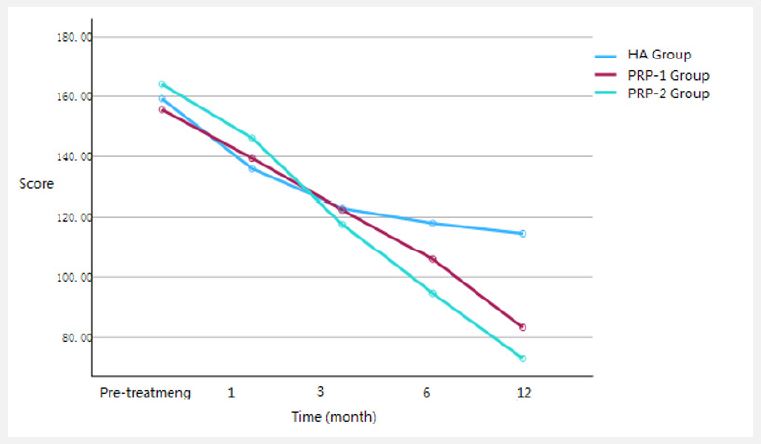
Comparison of WOMAC scores and overall efficacy
The WOMAC scores are summarized in Table 5 and Figure 2. At 1 and 3 months post-treatment, all three groups showed significant reductions in WOMAC scores compared to baseline (P< 0.05), with no significant differences among the groups. By 6 and 12 months, the WOMAC scores continued to decrease in all groups (P< 0.05). At 12 months, the PRP acupoint injection group achieved significantly lower WOMAC scores than both the PRP routine injection group (P2< 0.05) and the HA group (P3< 0.05). In terms of treatment efficacy, the PRP acupoint injection group achieved the best overall outcomes, with a total effective rate of 100%, compared to 90.47% in the PRP routine injection group and 43.47% in the HA group in Table 6 (P< 0.001).
| Group | Samplesize | Character | No. | Reason |
|---|---|---|---|---|
| HA group | 30 | Lost | 7 | Recurrent lossof patient follow-up/refusal to adhere to treatment. |
| Follow-up | 23 | -- | ||
| PRPjoint injection group | 30 | Lost | 9 | Recurrent loss of patient follow-up/contamination with potential PRP/refusal to adhere to treatment. |
| Follow-up | 21 | -- | ||
| PRP jointinjection combined withacupoint injection group | 30 | Lost | 4 | Recurrent loss of patient follow-up/contamination with potential PRP/refusal to adhere to treatment. |
| Follow-up | 26 | -- |
| group | Case | Man | Woman | Age | K-L1 scale | K-L2 scale | K-L3 scale |
|---|---|---|---|---|---|---|---|
| HA group | 23 | 10 | 13 | 52.74±0.83 | 8 | 8 | 7 |
| PRPjoint injection group | 21 | 9 | 12 | 52.66±1.02 | 8 | 9 | 4 |
| PRPjoint injection combined with acupoint injection group | 26 | 12 | 14 | 51.62±0.96 | 9 | 8 | 9 |
| Homogeneity of variance | 0.645 | 0.099 | 0.848 | ||||
| F | 0.117 | 0.409 | 0.361 | ||||
| P | 0.89 | 0.667 | 0.669 |
| VASscore results | t0 | t1 | t2 | t3 | t4 | F | P |
|---|---|---|---|---|---|---|---|
| HA gruop (n=23) | 6.6±0.98 | 4.57±0.75a | 3.75±0.74ab | 3.37±0.53ab | 3.59±0.5ab | 90 | <0.001 |
| PRPConventional group (n=21) | 6.61±0.77 | 4.72±0.96a | 3.7±0.6ab | 3.01±0.44abc | 2.74±0.35abcd | 111.45 | <0.001 |
| PRPCombination group (n=26) | 6.61±0.84 | 4.35±0.78a | 3.38±0.5ab | 2.7±0.59abc | 2.23±0.5abcd | 176.72 | <0.001 |
| F | 0.001 | 1.21 | 2.62 | 9.67 | 53.45 | ||
| P | 0.99 | 0.3 | 0.08 | <.001 | <.001 | ||
| P1 | 1 | 1 | 1 | 0.08 | <.001 | ||
| P2 | 1 | 1 | 0.12 | <.001 | <.001 | ||
| P3 | 1 | 0.38 | 0.23 | 0.15 | 0.001 | ||
| Ftime=692.67 Ptime<0.001 Fgroup=6.16 ,Pgroupg=0.003 Fgroup*time=7.93 Pgroup*time <0.01 | |||||||
a: A significant difference compared to baseline (before treatment), b: indicates a significant difference 1 month after treatment, c: represents a significant difference 3 months after treatment, and d: Denotes a significant difference 6 months after treatment. P1 refers to the significance of the comparison between the HA group and the PRP conventional group at the same time point. P2 indicates the significance of the comparison between the HA group and the PRP combined group at the same time point, while P3 represents the significance of the comparison between the PRP conventional group and the PRP combined group at the same time point.
| KSS scoreresults | t0 | t1 | t2 | t3 | t4 | F | P |
|---|---|---|---|---|---|---|---|
| HA gruop (n=23) | 139.13±5.61 | 159.48±4.76a | 164.22±6.37ab | 165.39±6.01ab | 158.78±4.02acd | 143.76 | <.001 |
| PRPConventional group (n=21) | 140.76±5.59 | 159.95±5.73a | 170.43±3.79ab | 173.86±4.35abc | 172.1±5.77ab | 181.21 | <.001 |
| PRPCombination group (n=26) | 142.15±5.66 | 161.77±4.4a | 174.58±5.09ab | 180.54±3.59abc | 178.38±4.14abc | 285.87 | <.001 |
| F | 1.76 | 1.47 | 24.14 | 62.74 | 111.22 | ||
| P | 0.17 | 0.23 | <.001 | <.001 | <.001 | ||
| P1 | 1 | 1 | <.001 | <.001 | <.001 | ||
| P2 | 0.19 | 0.33 | <.001 | <.001 | <.001 | ||
| P3 | 1 | 0.64 | 0.026 | <.001 | <.001 | ||
| Ftime=625.26 Ptime<0.001 Fgroup=63.04 Pgroup=<.001 Fgroup*time=18.48 Pgroup*time<0.01 | |||||||
a: Denotes a significant difference compared to baseline (before treatment). b: Indicates a significant difference 1 month after treatment, c: Represents a significant difference 3 months after treatment, and d: Denotes a significant difference 6 months after treatment. P1 refers to the significance of the comparison between the HA group and the PRP conventional group at the same time point. P2 indicates the significance of the comparison between the HA group and the PRP combined group at the same time point, while P3 represents the significance of the comparison between the PRP conventional group and the PRP combined group at the same time point.
| WOMAC scoreresults | t0 | t1 | t2 | t3 | t4 | F | P |
|---|---|---|---|---|---|---|---|
| HA gruop (n=23) | 159.26±11.91 | 135.91±9.68a | 122.91±18.53a | 118±17.35ab | 114.57±14.85ab | 86.86 | <0.001 |
| PRP conventional group (n=21) | 155.62±14.13 | 139.38±15.57a | 122.38±14.14ab | 105.86±14.69abc | 83.29±13.2abcd | 163.02 | <0.001 |
| PRP combination group (n=26) | 164.08±13.15 | 146.08±17.31a | 117.58±17.39ab | 94.65±14.88abc | 72.92±12.91abcd | 282.7 | <0.001 |
| F | 2.48 | 3.06 | 0.74 | 13.52 | 60.02 | ||
| P | 0.09 | 0.05 | 0.47 | <0.01 | <0.01 | ||
| P1 | 1 | 1 | 1 | 0.038 | <.001 | ||
| P2 | 0.607 | 0.054 | 0.821 | <.001 | <.001 | ||
| P3 | 0.092 | 0.054 | 1 | 0.053 | 0.036 | ||
| Ftime=467.19 Ptime <0.001 Fgroup=6.18 Pgroup=0.003 Fgroup*time=26.31 Pgroup*time <0.01 | |||||||
a: Denotes a significant difference compared to baseline (before treatment). b: Indicates a significant difference 1 month after treatment, c: Represents a significant difference 3 months after treatment, and d: Denotes a significant difference 6 months after treatment. P1 refers to the significance of the comparison between the HA group and the PRP conventional group at the same time point. P2 indicates the significance of the comparison between the HA group and the PRP combined group at the same time point, while P3 represents the significance of the comparison between the PRP conventional group and the PRP combined group at the same time point.
| Character | Apparent effect | Effective | Improve | Ineffective | Total effective rate |
|---|---|---|---|---|---|
| HAgroup (n=23) | 0 | 0 | 10 | 13 | 43.47% (10) |
| PRPConventional group (n=21) | 1 | 7 | 11 | 2 | 90.47% (19) |
| PRPCombination group (n=26) | 1 | 20 | 5 | 0 | 100% (26) |
| P | <0.001 |
Knee Osteoarthritis (KOA) is a common orthopedic condition characterized by progressive degenerative changes in the knee joint. Epidemiological data indicate a lifetime risk of developing KOA of approximately 40% in men and 47% in women. In China, the prevalence among individuals over the age of 60 is as high as 42.8% [9,10]. With an aging population and the increasing prevalence of obesity, the incidence of KOA is expected to rise further. Unfortunately, effective non-surgical treatments for early-stage KOA remain limited, often leading patients to total knee replacement. This surgical option imposes significant financial and physical burdens on both patients and society.
Treatment strategies for KOA can be broadly categorized into surgical and conservative approaches. Surgical interventions, such as total knee arthroplasty and osteotomy, are typically reserved for advanced cases. Conservative treatments include pharmacotherapy, physical therapy, novel physical interventions, intra-articular injections, and acupoint injections. However, surgical treatments are not universally suitable, and studies report that approximately 40% of patients continue to experience pain and swelling following total knee replacement [11].
Recent research has increasingly focused on non-surgical treatments for early- and mid-stage KOA to delay or even halt disease progression. Among these, autologous Platelet-Rich Plasma (PRP) therapy has emerged as a promising modality due to its safety and efficacy. Numerous studies have shown that PRP injections significantly alleviate pain, slow disease progression, promote chondrocyte proliferation, enhance cartilage regeneration, and reduce proinflammatory factors in the knee joint [12,13].
Acupoint injection therapy, which involves the administration of medications into specific acupuncture points, has also demonstrated efficacy in KOA management. Studies have identified several key acupoints, including Xuehai, Yanglingquan, and Weizhong, as effective in alleviating KOA-related pain. Xuehai is located two inches above the medial end of the patellar base on the anterior femoral region, corresponding to the Spleen meridian of Foot Taiyin. Yanglingquan is situated on the lateral calf below the fibular head and aligns with the Gallbladder meridian of Shaoyang. Weizhong is positioned in the popliteal fossa between the biceps femoris and semitendinosus tendons, associated with the Bladder meridian of Foot Taiyang [14-16]. Integrating traditional Chinese medicine approaches, such as acupuncture and cupping, with modern therapeutic modalities has shown promise in KOA management [17,18].
This study demonstrated that the combination of PRP intra-articular injections with acupoint injections at Xuehai, Yanglingquan, and Weizhong is superior to either PRP or Hyaluronic Acid (HA) injections alone. Patients receiving the combined treatment experienced significant improvements in VAS pain scores, WOMAC osteoarthritis index, and KSS joint function scores. These findings suggest that the combined therapy effectively alleviates pain, enhances joint function, and improves overall patient satisfaction.
Limitations
However, this study has limitations. The sample size was relatively small, and the follow-up period was limited. Future research should focus on larger cohorts and longer follow-up durations to confirm the safety and efficacy of this therapeutic approach.
In conclusion, PRP intra-articular injections combined with PRP acupoint injections at Xuehai, Yanglingquan, and Weizhong demonstrated significant therapeutic benefits for KOA. This combined approach represents a safe, effective, and promising option for improving joint function and achieving excellent long-term outcomes in KOA management.
Funding: Science and Technology Open Cooperation Project of Henan Academy of Sciences (Grant No. 220914011).
