1Department of Disease Control, School of Veterinary Medicine, University of Zambia, Lusaka Zambia.
2Department of Biomedical Sciences, School of Health Sciences, University of Zambia, Lusaka, Zambia.
3Macha Research Trust, Choma, Zambia.
4Department of Paraclinical Studies, School of Veterinary Medicine, University of Zambia, Lusaka, Zambia.
Martin Nyahoda
Email: martinny2@yahoo.co.uk
Received : Nov 27, 2024 Accepted : Dec 23, 2024 Published : Dec 30, 2024 Archived : www.meddiscoveries.org
Background: Respiratory infections are among the leading causes of morbidity and mortality globally especially in sub-Saharan Africa.
Objectives: The aim of this systematic review and meta-analysis was to compare the prevalence between viral and bacterial respiratory pathogens and determine the African regions with the highest burden of respiratory infections in order to help target public health interventions to African regions with the greatest need and achieve efficient utilization limited resources.
Methods: PubMed and Google Scholar were systematically searched for studies in Africa published between January 2013 and 28th September, 2023. Of the total 758 articles retrieved after removing duplicates, 39 studies were included in this review with a sample size of 72,196 with a representation of all age groups. Studies were grouped in 5 regions based on country of study, Southern, North, Central, East and West Africa.
Results: The majority of studies were from Southern Africa (20/39) while the Central Africa had the least with (2/39). With respect to age, children < 15 years accounted for the majority of studies with 59% (23/39) of the articles retrieved. Most studies (37/39, 94.9%) tested and reported viral respiratory aetiologies with (25/37), 67.6% of studies exclusively testing and reporting viral respiratory pathogens. Only (14/39), 35.9% studies tested and reported bacterial respiratory pathogens. Overall pooled prevalence for viral and bacterial respiratory aetiologies was estimated at 56.6% (95% CI, 0.371-0.762; I2 99.9%) and 21.5% (95% CI, 0.203-0.228; I2 99.96%) respectively. At continental level, rhinovirus and respiratory syncytial virus were the most predominant pathogens with a wide geographical spread across all African regions with 19.9% and 8.9% prevalence, respectively. North Africa was highest in RSV prevalence with 16.1% while Southern and Central Africa had the highest rhinovirus burden with 25.9% and 26.3% respectively. North Africa had the highest influenza burden with 28.2% with the least being Central Africa with 0.2% influenza prevalence. Streptococcus Pneumoniae was the commonly reported bacterial pathogen with the highest burden in Central Africa with 55.5% prevalence.
Conclusions: This study generated evidence that the burden of respiratory pathogens is highest in North and Southern Africa. Further, the majority of studies are focused on viral respiratory pathogens neglecting bacterial pathogens. To fully understand the burden of respiratory infections in Africa and improve prognosis, there is a need for more studies combining detection of both viral and bacterial respiratory pathogens.
Keywords: Respiratory infections; Burden; Africa; Viruses; Bacteria.
Estimates indicate that respiratory infections are among the top 10 leading causes of death in children aged 0-14 years especially in low and middle-income countries [1]. In 2019, global morbidity incidence associated with Lower Respiratory Tract Infections (LRTIs) was estimated to be 488.9 million with about 2.4 million deaths [2]. Sub-Saharan Africa accounts for 66.4 deaths attributable to LRTI per 100,000 persons which is considered the highest globally [3]. In African children, estimates show that 38.6% of infectious disease deaths and 14.9% of all deaths are caused by LRTI [1,4]. Epidemiological studies have further shown that co-infections of viral-bacterial pathogens may increase the severity of disease especially in immune compromised and TB patients leading to poor prognosis [5]. The incidence of LRTIs remains high in HIV-positive children even with the widespread use of antiretroviral therapy thereby increasing the risk of severe disease and death [6].
Both viral and bacterial pathogens have been implicated in LRTIs and associated with Community-Acquired Pneumonia (CAP). Among viral pathogens responsible for LRTI causing Influenza-Like Illnesses (ILI) and Severe Acute Respiratory Infections (SARI) include, Influenza, Parainfluenza Viruses (PIV), Respiratory Syncytial Virus (RSV), Rhinovirus, Human Bocavirus (HBoV) and Coronaviruses [7]. On the other hand, bacterial pathogens such as Haemophilus influenzae, Streptococcus pneumoniae, Staphylococcus aureus and Bordetella pertussis have been found to contribute to disease severity and poor patient outcomes in incidences of co-infections [8,9]. However, even with the advent of multiplex Polymerase Chain Reaction (PCR), most scientific studies have focused on viral respiratory pathogens neglecting the interactions between viral and bacterial respiratory pathogens in causing severe respiratory illnesses and death. It is important to acknowledge that viral infections predispose to the growth of bacterial pathogens leading to a high risk of pneumonia.8 Therefore, studies on the aetiology of viral or bacterial respiratory infections do not need to be mutually exclusive but holistic encompassing both viral and bacterial pathogens to implement interventions that improve prognosis.
With interventions being implemented for prevention and treatment such as vaccination and antibiotic use in the management of LRTI, it is important to evaluate their impact and effectiveness in the light of well-documented scientific evidence and determine geographical disparities [10]. Tracking the geographical distribution of disease helps in planning targeted interventions resulting in better utilization of limited resources [10]. This systematic review and meta-analysis was therefore aimed at establishing the geographical distribution and prevalence of viral and bacterial respiratory infections in Africa.
In undertaking this systematic review and meta-analysis, the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) were followed. The systematic review was not registered to the International Prospective Register of Systematic Reviews (PROSPERO).
Search strategy and eligibility criteria
Pubmed and Google Scholar were systematically searched for epidemiological studies published between January 2013 and 28th September, 2023 in English language. Search terms were a combination of three key concepts; respiratory pathogens, prevalence and co-infections. To bolster the search, the key concepts were coupled with similar or related words such as “co-infections” OR “dual infections”, OR “multiple infections” OR “Lower respiratory infections” OR “upper respiratory infections”.
Molecular studies with multiple detections of respiratory pathogens were included. In terms of geographical coverage, only studies from Africa were included. Only studies with sample specimens collected from humans were included. Additionally, the review included only articles from original studies. Among studies excluded were serological studies, epidemiological studies done outside the African region, specimens collected from non-humans and systematic reviews, conference proceedings and dissertations.
Data abstraction and analysis
Using a predefined template in Microsoft Excel, data was extracted based on author, study title, year of publication and country where the study was conducted. Sample size, method of detection and specimen type (oral or nasopharyngeal swabs) were also abstracted from eligible studies. The prevalence of infection for each pathogen detected was recorded together with information on co-infections that were detected. Data Analysis to estimate pooled prevalence and construction of forest plots was performed in OpenMeta (OSX: Yosemite 10.10, USA). Heterogeneity was assessed as described by Krumbein et al, 2022 [11].
Outcomes
The main outcome of this systematic review and meta-analysis was a comparative prevalence of various aetiologies for respiratory infections in different African regions. Additionally, the review sought to determine the geographical distribution of both viral and bacterial respiratory pathogens across the African continent, revealing geographical disparities and regions with a high burden.
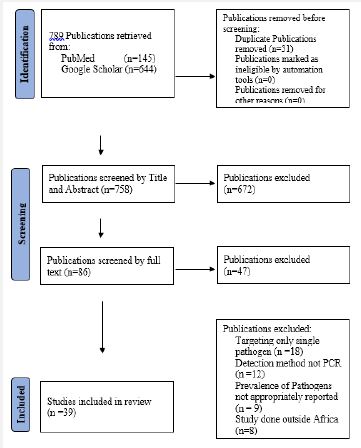
After a systematic search in PubMed and Google Scholar, 789 publications were retrieved as shown in Figure 1. After deduplication in endnote 21 version 21.2, seven hundred and fifty-eight publications were available for screening. After title screening, 613 publications were excluded remaining with 145 publications. After reviewing abstracts, 59 publications were excluded. After full-text screening, 39 publications were included in the systematic review and meta-analysis with a total sample size of 72,196.
Characteristics of included studies.
All studies included were conducted using either nasopharyngeal or oropharyngeal specimens with multiplex RT-PCR as the detection method. Studies were clustered in 5 regions as Southern Africa, West Africa, East Africa, North Africa and Central Africa to enable regional comparisons on the distribution and prevalence for respiratory pathogens of interest. Southern Africa had the most publications with 20 followed by West Africa with 12. East Africa had 4 publications while North Africa and Central Africa had the least number of publications with 2 each. The majority of studies (23/39), 59% were conducted in children <15 years with children <5 years accounting for the majority (18/23), 78% of studies. Although the majority of studies were in children, overall, all age groups were represented in the included studies. All studies except 2 had sample sizes of more than 100 specimens with a highest sample size of 18,282 in a single study.
Overall prevalence of respiratory pathogens
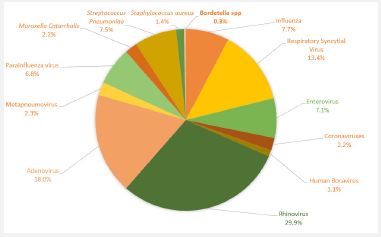
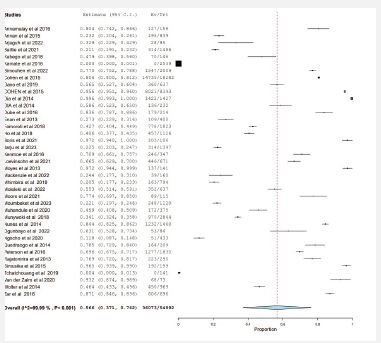
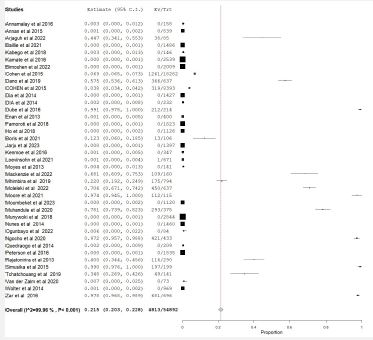
After analysis of a total sample of 72,196 specimens, viral respiratory pathogens accounted for a larger proportion of positive specimens than the bacterial. The pooled prevalence for respiratory viral infections was 56.6%, (CI, 0.371-0.762, I2 99.9%) for specimens testing positive for at least one pathogen (Figure 3). Bacterial respiratory pathogens had an estimated pooled prevalence of 21.5% (CI 0.203-0.223, I2 99.96%) of specimens testing positive for at least one pathogen, Figure 4. Among viral respiratory pathogens, Rhinovirus had the highest proportion of specimens positive accounting for 29.9% (Figure 2) with a prevalence of 19.9% (Table 1). Adenovirus and Respiratory Syncytial Virus (RSV) were second and third with 18% and 13.4% of the total specimens respectively and a prevalence of 12% and 8.9% respectively. Human Bocavirus was the least prevalent viral respiratory pathogen with only 1.1% proportion of the total specimens testing positive and a prevalence of 0.7%. For bacterial pathogens, Streptococcus pneumonia had the highest prevalence with a 7.5% proportion of specimens testing positive and a prevalence of 5% followed by Moraxella catarrhalis with 2.2% and a prevalence of 1.5%.
Regional prevalence comparisons for detected respiratory pathogens
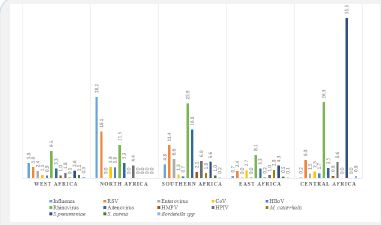
After analyzing regional prevalence, clustered as Southern, Central, North, East and West Africa, the prevalence of influenza was predominant in North Africa with 28.2% followed by West Africa with 5.3% (Figure 5). Rhinovirus was most prevalent in Southern Africa with 25.9% followed by Central Africa with 26.3% (Figure 5). East Africa recorded the least Rhinovirus prevalence with 8.1%. Respiratory Syncytial Virus (RSV) was highest in North Africa with a prevalence of 16.1% followed by Southern Africa with 11.4%. East Africa recorded the least RSV prevalence estimated at 2.4%. Human Adenovirus was highest in South ern Africa with an estimated prevalence of 16.8%. Overall, few bacterial respiratory infections were recorded in North Africa compared to the rest of the regions. Central Africa recorded the highest Streptococcus pneumoniae prevalence with 55.5% while the lowest was North Africa which did not record any streptococcus pneumoniae infections. East Africa accounted for the highest proportion of Moraxella catarrhalis with 2.8% followed by Southern Africa with 1.8%.
| Pathogen | Specimenspositive | %Prevalence (N=72196) |
|---|---|---|
| Influenza | 3730 | 5.2 |
| RSV | 6447 | 8.9 |
| Enterovirus | 3407 | 4.7 |
| CoV | 1080 | 1.5 |
| HBoV | 533 | 0.7 |
| Rhinovirus | 14401 | 19.9 |
| Adenovirus | 8664 | 12.0 |
| HMPV | 1118 | 1.5 |
| HPIV | 3263 | 4.5 |
| M.catarrhalis | 1062 | 1.5 |
| S.pneumoniae | 3619 | 5.0 |
| S.aureus | 666 | 0.9 |
| Bordetella spp | 168 | 0.2 |
| Total | 48158 |
Age group comparisons for detected respiratory pathogens
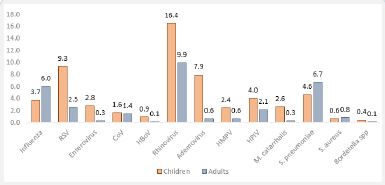
Results for age group comparisons (Figure 6), revealed that children accounted for a greater proportion of both viral and bacterial respiratory infections than adults. More specifically, Rhinovirus had an estimated prevalence of 16.4% in children while it was 9.9% in adults. RSV had an estimated prevalence of 9.3% in children and 2.5% in adults. For bacteria, the prevalence of M. catarrhalis was estimated to be 2.6% in children while it was 0.3% in adults. S. pneumoniae infection was higher in adults with 6.7% prevalence than in children with 4.6%.
This systematic review and meta-analysis was aimed at estimating the prevalence of viral and bacterial respiratory pathogens and making regional geographical comparisons to determine African regions with high a burden of respiratory infections between 2013 and 2023. This information is important in order to target public health interventions to most needed areas and ensure better utilization of resources [10]. This study revealed that epidemiological studies have to a large extent focused on elucidating viral aetiologies for respiratory infections in Africa with little attention paid to bacterial pathogens. This could help explain the high prevalence of viral respiratory aetiologies compared to bacterial respiratory aetiologies observed in the review. The high prevalence of Rhinovirus observed in the studies in this review agrees with other scientific literature which have shown that Rhinoviruses are the leading cause of acute respiratory infections and represent a substantial proportion of the global burden of upper respiratory infections [12,13]. While little attention has been paid to the role of adenovirus in both upper and lower respiratory tract infections and severe disease, this review seems to suggest that its prevalence may be significant in the pathogenesis of respiratory infections especially in cases of co-infections as demonstrated by other studies [11].
Comparing the results of this review on influenza prevalence with the World Health Organization (WHO) epidemiological data on influenza in Africa revealed that the results of this study were similar. Influenza prevalence was highest in North and Southern Africa with 28.2% and 5.3% respectively, consistent with WHO epidemiological data which has shown highest influenza prevalence in North and Southern Africa [14].
In this study, the prevalence of Respiratory Syncytial Virus (RSV) was highest in North Africa with 16.1% followed by Southern Africa with 11.4% consistent with results of a systematic review and meta-analysis by Regassa et al 2023 [15], on the molecular epidemiology of respiratory syncytial virus in children with acute respiratory illnesses in Africa in which sub-regional analysis revealed that North and Southern Africa had the highest prevalence of RSV.
These results show that North and Southern Africa may be the regions with the highest burden of RSV in Africa. Further, this study revealed that Central and Southern Africa have the highest burden of Rhinovirus with 26.3% and 25.9% prevalence respectively. Public health interventions targeting reduction of the burden of disease from these respiratory infections should be more considered in these regions of Africa.
Epidemiological studies have revealed that opportunistic bacterial infections especially M. catarrhalis have been implicated in causing otitis media and acute exacerbations of Chronic Obstructive Pulmonary Disease (COPD) in children and adults with co-infections resulting in adverse prognosis [16]. With this study showing a high burden of S. pneumoniae and M. catarrhalis in Central and Southern Africa, improving patient outcomes from these respiratory infections especially in cases of co-infections with viral pathogens may require preventive programs that limit exposure to these respiratory infections in these regions.
Generally, although bacterial respiratory pathogens play a major role in the pathogenesis of upper and lower respiratory tract infections especially in incidences of viral-bacterial co-infections resulting in poor patient outcomes, results of this study have shown that little attention is paid in undertaking epidemiological studies focusing on bacterial respiratory pathogens [11,17,18]. With the advent of multiplex polymerase chain reaction, studies focusing on simultaneous detection of both viral and bacterial respiratory pathogens and elucidating their impact on disease severity should be encouraged especially in Africa. This is necessary in designing intervention efforts for prevention and mitigating effects of viral-bacterial interactions that may result in severe disease outcomes.
As other studies have shown this review demonstrated that the burden of both viral and bacterial respiratory pathogens is higher in children than in adults [7,11].
This systematic review and meta-analysis provides evidence that the burden of respiratory viral infections is highest in North and Southern Africa. In terms of both viral and bacterial respiratory pathogens considered together, Southern Africa has the highest burden of infection. For bacterial respiratory pathogens alone, North Africa has the lowest burden of infection. This review provides further evidence that there are few studies conducted targeting multiplex testing for co-detection of viral and bacterial respiratory pathogens especially in East and Central Africa.
Most studies are focused on viral respiratory pathogens. Considering the impact of viral-bacterial co-infections on the pathogenesis of respiratory infections and prognosis, there is need for more studies focusing on co-detection of viral and bacterial respiratory pathogens to clearly understand the burden of respiratory infections in Africa and help target interventions to improve patient outcomes.
Competing interests: The authors declare no competing interests.
Author contributions: MN and ES conceptualized the study. MN and AN performed the search, analyzed the data and drafted the manuscript. NS, ES and KC substantially revised the draft manuscript.
Acknowledgements: The authors are grateful to Chitalu Wedex Ilunga for technical assistance in figure presentation.
