1Department of Oncology, Tishreen University Hospital, Latakia, Syria.
2Department of Vascular Surgery, Tishreen University Hospital, Latakia, Syria.
3Department of Pathology, Tishreen University Hospital- Lattakia- Syria.
Duaa Knaj
Email: duaa.knaj@tishreen.edu.sy
Received : Nov 23, 2024 Accepted : Dec 20, 2024 Published : Dec 27, 2024 Archived : www.meddiscoveries.org
Background: Intramuscular vascular malformations are benign malformations of skeletal muscle vessels. These rare tumors can cause significant symptoms and should be accurate diagnosed.
Case presentation: A 25-year-old Syrian woman presented in 2015 with dyspnea and difficulty speaking. She had a mass under the angle of the left mandible, over which the skin was intact. The mass started small a year ago and gradually increased in size and symptoms until she presented with the previous symptoms. An ultrasound examination revealed a mass measuring 4 × 5 × 6 cm on the left aspect of the neck, associated with lymph node enlargement. A contrast-enhanced computed tomography showed a mass of heterogeneous density, pushing the tongue upward and to the right. The mass was found to be adherent to the left mandible and to the sub-maxillary branch of the left external carotid artery, without evidence of bone destruction. The mass appeared to be hypervascular. Total resection of the mass was achieved by surgery. Pathological examination revealed an IVM of the hyoglossus muscle. There was no recurrence or return of symptoms during follow-up for nine years following surgery.
Conclusion: Careful clinical assessment, an accurate anatomical study of the relevant structures and appropriate imaging modalities are essential for the accurate diagnosis of any mass in the head and neck region.
Keywords: IVM; Skeletal; Hyoglossus muscle; Case report.
Intramuscular Vascular Malformations (IVMs) are primarily congenital anomalies characterized by abnormal blood vessel formations within muscle tissue [1]. They are present at birth, with potential for sudden enlargement. They may remain asymptomatic until complications arise [2]. IVMs are initially classified into several types based on the dominant vessel involved, clinical manifestations, and treatment strategies. The major types of IVM according to the International Society for the Study of Vascular Anomalies (ISSVA) classification include venous malformations, capillary malformations, lymphatic malmalformations, arteriovenous malformations, and combined malformations consisting of more than one vessel type [3].
A 25-year-old Syrian woman presented to our hospital in 2015 with difficulty speaking and shortness of breath. On clinical examination, the patient was in a moderate general condition, with a clear mass under the angle of the left mandible, measuring approximately 6 cm; the overlying skin was intact. One year ago, the mass started small and gradually increased in size during this period, associated with an increase in symptoms, until she presented with the previous symptoms. She had no surgical or medical history. Ultrasound showed a 4 × 5 × 6 cm mass on the left aspect of the neck with enlargement of the left lymph node. A contrast-enhanced Computed Tomography (CT) scan with contrast was performed and showed the previous mass pushing the tongue upward and to the right, adhering to the left mandible and the submandibular branch of the left external carotid artery without bone destruction (Figure 1). The mass was very close to the airway at the level of the oropharynx. It appeared with heterogeneous density, relatively low. The left cervical lymph nodes appeared enlarged. The mass seemed to be hypervascular.

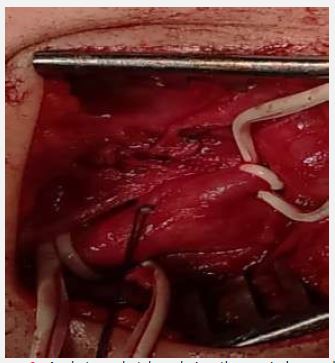

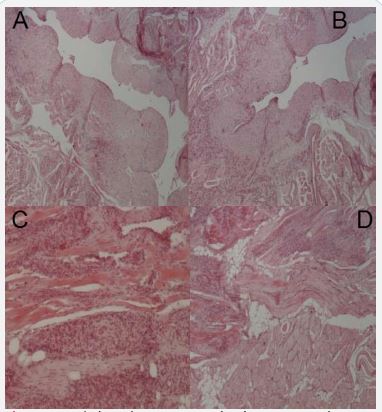
The patient was referred to the surgical department and it was decided to perform resection with the intention of complete removal of the mass with preservation of adjacent structures. Surgery was performed under general anesthesia. During surgery, the mass appeared large, soft, with clear borders at the base of the tongue and the floor of the mouth, pressing the tongue and the oropharynx from the left side. It was within the thickness of the hyoglossus muscle. The surgeon performed a complete resection of the affected muscle with an enlarged cervical lymph node (Figures 2,3). The surgical specimens were sent to the pathology department for histopathological examination. Macroscopically, the specimen was a 5 × 4.5 × 2 cm solid gray mass surrounded by a capsule (Figure 4).
A microscopic examination revealed the presence of a benign proliferation of vascular endothelial cells between striated muscle fibers, with vascular formations of varying sizes, including large, medium, and small capillaries. The cells were observed within a small, highly degraded matrix, which was a consequence of the inflammatory response associated with degenerative changes in skeletal muscle under the pressure of tumor growth. The vessels exhibited a range of wall thicknesses. Endothelial cell proliferation was the predominant phenomenon. An enlarged lymph node demonstrated reactive lymphoid hyperplasia, follicular type, which was caused by the inflammatory reaction of the degenerative changes (Figure 4). On the basis of radiological, surgical and histological findings, the tumor was diagnosed as an IVM of the hyoglossus muscle. Following surgical intervention, the patient’s general condition showed marked improvement with regard to respiration, swallowing, and speech. Following treatment, the patient was monitored on a regular basis, initially at three-month intervals for the first year, then at six-month intervals for the second year, and subsequently at annual intervals for a period of nine years, through a combination of clinical evaluation and ultrasound. As of the time of writing this report, after nine years, there has been no recurrence or return of symptoms.
Intramuscular vascular malformations are rare lesions that can occur in various muscles, with a notable prevalence in the head and neck region [4]. These malformations can cause significant clinical symptoms in patients, including pain, swelling, and functional impairment. Therefore, an accurate diagnosis is essential for the appropriate management of these conditions. Diagnosis is based on history, clinical examination, and the use of appropriate imaging techniques. Imaging is a crucial tool in the diagnosis and management of intramuscular vascular malformations. Ultrasound (US) plays an important role in the diagnosis of IVMs. The advantages of US include real-time imaging, non-invasiveness, and cost-effectiveness, making it a preferred initial diagnostic tool [5].
Magnetic Resonance Imaging (MRI) is the preferred modality due to its superior soft tissue contrast and ability to provide multiplanar views [6]. Computed Tomography (CT) is a valuable tool for evaluating the relationship between the malformations and surrounding structures [7]. Doppler Ultrasound (DUS) can help evaluate blood flow characteristics, aiding in differentiating between different types of vascular malformations. In the present study, MRI was unable, but CT and US were made for imaging.
We present a rare case of an intramuscular vascular malformation in the hyoglossus muscle, where complete resection of the mass resulted in a prolonged period of follow-up without any recurrence. Given the potential for these tumors to cause cosmetic or functional impairment, accurate management is recommended. Furthermore, long-term follow-up is crucial for the early detection of potential recurrence and the assurance of optimal outcomes following treatment.
