1Intensive Care Unit, People’s Hospital of Qiandongnan Miao and Dong Autonomous Prefecture, Kaili 556000, Guizhou, China.
2Obstetrics, People’s Hospital of Qiandongnan Miao and Dong Autonomous Prefecture, Kaili 556000, Guizhou, China.
Ling Wang
Email: 463082910@qq.com
Received : Nov 18, 2024 Accepted : Dec 13, 2024 Published : Dec 20, 2024 Archived : www.meddiscoveries.org
Uterine atony can prolong labor or lead to postpartum hemorrhage, posing a threat to maternal life. Predicting uterine atony prenatally is crucial for choosing delivery methods and formulating emergency strategies. This study aimed to identify key factors affecting uterine atony using a neural network model to guide clinical management. We retrospectively analyzed 23,490 cases, finding that uterine atony occurred in 14.29% (3,356/23,490) of deliveries, with postpartum hemorrhage (31.29%; 1050/3356) being the most common complication. Uterine extirpation was necessary in 2.21% (74/3356) of atony cases. A neural network model with one hidden layer and eight neurons achieved a prediction accuracy of 86.3% for both the training and testing sets. Model analysis revealed that placenta accreta (100.0% importance), retained placenta (79.7% importance), age (68.7% importance), and placenta previa (65.3% importance) were the most significant factors affecting uterine atony. This study demonstrates the effectiveness of the constructed neural network model in predicting uterine atony. The findings highlight the potential critical role of placenta accreta, retained placenta, age, and placenta previa in uterine atony development, informing clinical decision-making.
Keywords: Uterine atony; Risk factors; Prediction; Model; Postpartum hemorrhage.
During childbirth, physiological contractions of the uterus are essential for expelling the fetus through the birth canal and controlling Postpartum Hemorrhage (PPH). However, inadequate contractions, termed as Uterine Atony (UA), can occur. UA is a common and increasingly prevalent obstetric complication characterized by an insufficient response of the uterine muscle cells to endogenous oxytocin released during labor [1,2]. This complication can prolong labor and increase the risk of PPH. Studies have indicated that UA is the most common cause of maternal mortality due to PPH [3-7], posing a serious threat to maternal life. Therefore, predicting and understanding the factors influencing UA are crucial for developing personalized treatment strategies and preventing PPH.
Multiple factors contribute to UA development. In recent years, neural networks have emerged as powerful tools in the medical field [8]. These models can effectively analyze large datasets of clinical information to identify underlying patterns and relationships between variables [9]. This study employs an iterative neural network model to analyze the relative importance of various factors influencing UA development, aiming to provide valuable insights for clinicians in formulating optimal treatment plans.
The study adhered to the ethical principles outlined in the revised 2013 Declaration of Helsinki 1975 and followed the STROBE guidelines for reporting observational studies [10].
Study population
We conducted a retrospective study analyzing data from patients hospitalized for pregnancy requiring delivery at the People’s Hospital of Qiandongnan Miao and Dong Autonomous Prefecture from January 1, 2018, to December 31, 2023 (continuous case selection). Patients aged 18 years or older were included. We excluded six patients transferred for delivery elsewhere, one with PPH complicated by placental implantation, and 15 with missing records. This resulted in a final sample of 23,490 patients with a mean age of 31.00 ± 5.59 years. Among them, 3,356 (14.29%) experienced UA. Of these, 2,306 occurred during labor, 1,050 postpartum, and 1,050 involved PPH, representing 31.29% of all UA cases. Additionally, 74 patients (2.21%) with UA underwent hysterectomy, 13,526 underwent cesarean section, 399 underwent uterine artery embolization, and 5 died.
Diagnostic criteria for UA
We diagnosed UA based on insufficient uterine contractility during labor or decreased uterine involution postpartum. After excluding pelvic, fetal, and psychological factors, UA was defined by weak and ineffective contractions with normal polarity, symmetry, and rhythm but short duration, long intervals, or irregularity; this could lead to delayed or arrested labor (latent phase exceeding 16 hours in primiparous women or 8 hours in multiparous women; active phase cervical dilation rate <1.2 cm/h or <1.5 cm/h in multiparous women; second stage exceeding 2 hours in primiparous women or 1 hour in multiparous women). Postpartum UA was defined as excessive postpartum bleeding due to weak uterine contractions, excluding retained placenta, placental implantation, birth canal lacerations, and coagulation abnormalities.
Treatment methods
Cesarean section was performed in cases of cephalopelvic disproportion or abnormal fetal presentation. For diagnosing UA, treatment included continuous intravenous oxytocin infusion (1.2-2.4 U/h) and sustained uterine massage. Postpartum, Intramuscular Oxytocin Injection (10U) into the uterine fundus was administered. In cases of PPH, hemostatic measures tailored to the cause were promptly initiated, along with supportive therapies such as immediate intravenous administration of 1 g of tranexamic acid, early fluid resuscitation, and blood transfusion to maintain hemodynamic stability. Additional interventions like pelvic and vaginal packing, pelvic vessel ligation, transcatheter uterine artery embolization, and uterine extirpation were performed when needed, following established guidelines for PPH management in China [11].
Data collection and grouping
Data were collected from patient discharge health records and independently verified by at least three researchers for accuracy. Variables included age, number of pregnancies, number of deliveries, history of adverse obstetric or perinatal events, history of pelvic inflammatory disease, history of endometrial infections, history of vaginitis, history of cesarean section, pre-existing conditions (such as hypertension, diabetes), pregnancy complications (such as pre-eclampsia, hypertension, diabetes, cardiomyopathy), thrombocytopenia, intrahepatic cholestasis of pregnancy, uterine fibroids, overdue pregnancy, macrosomia, non-cephalic presentation, twin gestation, stillbirth, nuchal cord, polyhydramnios, oligohydramnios, premature rupture of membranes, placenta previa, retained placenta, placenta accreta, placental adhesion, placental abruption, and induced labor. Based on the presence or absence of UA during labor, patients were categorized into the UA and non-UA groups.
Statistical analysis
Statistical analyses were performed using SPSS 26.0 software. Continuous variables are presented as mean ± standard deviation, with intergroup comparisons performed using independent sample t-tests. Categorical data were analyzed using the χ² test. P<0.05 was considered statistically significant. To assess the importance of various factors influencing UA occurrence, we employed a multilayer perceptron neural network model. This model was constructed and evaluated repeatedly. The significance level for a factor’s importance was set at greater than 60% based on the neural network output.
Comparison of clinical data between the groups
We compared clinical characteristics between patients in the UA group and those in non-UA group. Patients in the UA group were older and had a higher number of previous deliveries than those in the non-UA group (t=11.500, 4.173, P<0.05). The UA group also exhibited higher rates of assisted reproductive technology use (χ²=16.425), prior pelvic inflammatory disease (χ²=116.168), endometrial infections (χ²=34.256), cesarean sections (χ²=188.892), pre-eclampsia (χ²=4.152), pre-pregnancy (χ²=18.704) or gestational (χ²=15.099) diabetes, peripartum cardiomyopathy (χ²=3.883), thrombocytopenia (χ²=17.814), uterine fibroids (χ²=13.663), macrosomia (χ²=24.290), non-cephalic presentation (χ²=138.020), twin pregnancy (χ²=84.606), stillbirth (χ²=5.164), polyhydramnios (χ²=14.541), placenta previa (χ²=634.447), retained placenta (χ²=25.230), placenta accreta (χ²=467.956), placental adhesion (χ²=7.927), placental abruption (χ²=10.563), and induced labor (χ²=53.107) than the non-UA group (all P<0.05). Conversely, the UA group had lower incidences of overdue pregnancy (χ²=11.681) and premature rupture of membranes (χ²=40.288) than the non-UA group (both P<0.05). Details are provided in Table 1.
Establishment of the multilayer perceptron neural network model
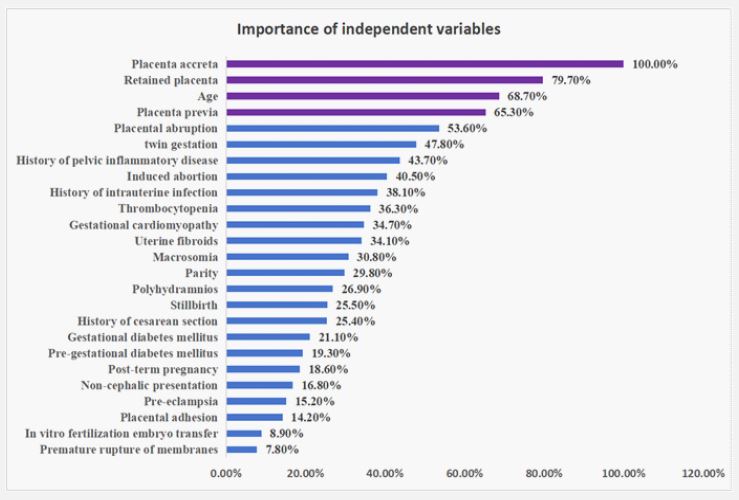
We employed a multilayer perceptron neural network to analyze factors influencing UA. All dependent variables were standardized for the model (categorical variables assigned 1 for yes and 0 for no). The model’s input layer statistically significant indicators (P<0.05) from Table 1, identified through correlation analysis. The output layer represented UA occurrence (assigned values: UA=1, non-UA=0). The number of nodes in the hidden layer and the activation function (chosen as the hyperbolic tangent) were automatically determined. The dataset was randomly divided into training (70%) and testing (30%) sets using a computer program. Batch processing and the conjugate gradient method were used for training. The model generated importance values for each factor, ranked in the descending order for convenience of analysis. Finally, a neural network model with one hidden layer and eight neurons was established, which achieved a prediction accuracy of 86.3% for both the training and testing sets. Placental accreta (100.0%), retained placenta (79.7%), age (68.7%), and placenta previa (65.3%) were identified as the most crucial factors influencing UA, with all importance values exceeding 60.0% (Table 2, Table 3, Figure 1).
| Parameters | Uterine atony group (n=3356) | Non-uterine atony group (n=20134) | χ2/t | P-value |
|---|---|---|---|---|
| Age in year,mean ± SD | 32.16±5.72 | 30.94±5.55 | 11.500 | 0.000 |
| Number of pregnancies, n (mean ± SD) | 3.57±3.32 | 2.98±2.35 | 1.244 | 0.214 |
| Number of deliveries, n (mean ± SD) | 1.52±0.99 | 1.45±0.93 | 4.173 | 0.000 |
| Assisted reproductive technology, n (%) | 249 (7.42) | 1125 (5.59) | 16.452 | 0.000 |
| History of adverse obstetric or perinatal events, n (%) | 631 (18.80) | 3608 (17.92) | 1.500 | 0.221 |
| History of pelvicinflammatory disease, n (%) | 304 (9.06) | 864 (4.29) | 116.168 | 0.000 |
| History of endometrial infections, n (%) | 129 (3.84) | 418 (2.08) | 34.256 | 0.000 |
| History of vaginitis, n (%) | 230 (6.85) | 1475 (7.33) | 0.968 | 0.325 |
| History of cesarean section, n (%) | 1400 (41.72) | 5957 (29.59) | 188.892 | 0.000 |
| Pre-pregnancy hypertension, n (%) | 139 (4.14) | 720 (3.58) | 2.527 | 0.112 |
| Gestational hypertension, n (%) | 90 (2.68) | 460 (2.28) | 1.911 | 0.167 |
| Pre-eclampsia, n (%) | 179 (5.33) | 910 (4.52) | 4.152 | 0.042 |
| Pre-pregnancy diabetes, n (%) | 342 (10.19) | 1593 (7.91) | 18.704 | 0.000 |
| Gestational diabetes, n (%) | 315 (9.39) | 1491 (7.41) | 15.099 | 0.000 |
| Peripartum cardiomyopathy, n (%) | 13 (0.39) | 40 (0.20) | 3.883 | 0.049 |
| Thrombocytopenia, n (%) | 61 (1.82) | 190 (0.94) | 17.814 | 0.000 |
| Intrahepatic cholestasis of pregnancy, n (%) | 83 (2.47) | 538 (2.67) | 0.450 | 0.502 |
| Uterine fibroids, n (%) | 73 (2.18) | 263 (1.31) | 13.663 | 0.000 |
| Overdue pregnancy, n (%) | 483 (14.39) | 3272 (16.25) | 11.681 | 0.003 |
| Macrosomia, n (%) | 168 (5.01) | 651 (3.23) | 24.290 | 0.000 |
| Non-cephalic presentation, n(%) | 1234 (36.77) | 5376 (26.7) | 138.020 | 0.000 |
| twin gestation, n(%) | 251 (7.48) | 751 (3.73) | 84.606 | 0.000 |
| Stillbirth, n (%) | 31 (0.92) | 115 (0.57) | 5.164 | 0.023 |
| Nuchal cord, n (%) | 898 (26.76) | 5290 (26.27) | 0.346 | 0.556 |
| Polyhydramnios, n (%) | 41 (1.22) | 118 (0.59) | 14.541 | 0.000 |
| Oligohydramnios, n (%) | 197 (5.87) | 1334 (6.63) | 2.768 | 0.096 |
| Premature rupture of membranes, n (%) | 376 (11.2) | 3074 (15.27) | 40.288 | 0.000 |
| Placenta previa, n(%) | 551 (16.42) | 773 (3.84) | 634.447 | 0.000 |
| Retained placenta, n (%) | 9 (0.27) | 2 (0.01) | 25.230 | 0.000 |
| Placenta accreta, n(%) | 205 (6.11) | 92 (0.46) | 467.956 | 0.000 |
| Placenta adhesion, n (%) | 2016 (60.07) | 11574 (57.48) | 7.927 | 0.005 |
| Placental abruption, n (%) | 33 (0.98) | 99 (0.49) | 10.563 | 0.001 |
| Induced labor, n (%) | 201 (5.99) | 656 (3.26) | 53.107 | 0.000 |
| Samples | Measured results | Predicted results | ||
|---|---|---|---|---|
| Non-uterine atonygroup | Uterine atony group | Correct percentage (%) | ||
| Training set | Non-uterine atony group | 13947 | 137 | 99.0% |
| Uterine atony group | 2113 | 242 | 10.3% | |
| Total percentage | 97.7% | 2.3% | 86.3% | |
| Test set | Non-uterine atony group | 5943 | 67 | 98.9% |
| Uterine atony group | 890 | 103 | 10.4% | |
| Total percentage | 97.6% | 2.4% | 86.3% | |
| Dependent variable: Uterine atony. | ||||
| Parameters | Importance | Importance of standardization (%) |
|---|---|---|
| Age | 0.076 | 68.7% |
| Parity | 0.033 | 29.8% |
| In vitrofertilization embryo transfer | 0.010 | 8.9% |
| History of pelvic inflammatory disease | 0.048 | 43.7% |
| History of intrauterine infection | 0.042 | 38.1% |
| History of cesarean section | 0.028 | 25.4% |
| Pre-eclampsia | 0.017 | 15.2% |
| Pre-gestational diabetes mellitus | 0.021 | 19.3% |
| Gestational diabetes mellitus | 0.023 | 21.1% |
| Gestational cardiomyopathy | 0.038 | 34.7% |
| Thrombocytopenia | 0.040 | 36.3% |
| Uterine fibroids | 0.038 | 34.1% |
| Post-term pregnancy | 0.021 | 18.6% |
| Macrosomia | 0.034 | 30.8% |
| Non-cephalic presentation | 0.019 | 16.8% |
| twin gestation | 0.053 | 47.8% |
| Stillbirth | 0.028 | 25.5% |
| Polyhydramnios | 0.030 | 26.9% |
| Premature ruptureof membranes | 0.009 | 7.8% |
| Placenta previa | 0.072 | 65.3% |
| Retained placenta | 0.088 | 79.7% |
| Placenta accreta | 0.111 | 100.0% |
| Placental adhesion | 0.016 | 14.2% |
| Placental abruption | 0.059 | 53.6% |
| Induced abortion | 0.045 | 40.5% |
UA is a major global contributor to the rising incidence of PPH [12-14]. Studies have shown that UA is a leading cause of hysterectomy, accounting for 27.0% of cases [15]. These findings highlight the significant impact of UA on maternal health outcomes. Despite advancements in medical technology and prenatal care, factors such as advanced maternal age, societal influences, and rising cesarean section rates may introduce new trends and contribute to UA development. Our study observed a UA incidence of 14.29%, with 31.29% of these cases progressing to PPH, further emphasizing the link between UA and PPH risk.
Several factors contribute to UA development [16,17]. Early identification and management of these risk factors are crucial for reducing PPH and maternal mortality risks. Our findings align with previous research by Ende et al. [18], indicating that primary factors influencing UA include age, parity, conception method, complications, history of cesarean section, fetal factors, polyhydramnios, placental factors, and post-term pregnancy. Notably, our analysis using a neural network model revealed that placental implantation (100.0% importance), retained placenta (79.7%), age (68.7%), and placenta previa (65.3%) were the most significant factors influencing UA, all exceeding 60% importance, aligning with prior findings [19]. Additionally, research suggests that placental issues are the primary causes of UA and subsequent PPH [20-23], further supporting our conclusions. The prominent role of placental factors underscores their importance when formulating clinical treatment strategies.
While this study identified placental factors as significant contributors to UA, offering valuable insights for clinical understanding and prevention of PPH, it is important to acknowledge the study’s limitations. The study’s single-center observation design, initial lack of sample size estimation, and specific demographics of the region (primarily Miao and Dong ethnic minorities) might introduce regional and ethnic variations in the data. Future research could benefit from larger, multicenter studies integrated with clinical practice for validation purposes.
This study employed a neural network model to comprehensively analyze factors influencing UA, highlighting the critical role of placental complications. Increased vigilance during the antenatal and peripartum periods is crucial for identifying at-risk pregnant women and implementing early interventions. These findings provide valuable insights for clinicians to develop more personalized treatment strategies for UA.
Competing interests: All authors declare that there is no conflict of interest.
Funding: Supported by Qiandongnan Prefecture Science and Technology Support Plan ([2021]11) and Training of High level Innovative Talents in Guizhou Province ([2022]201701)
