1Neijiang Traditional Chinese Medicine Hospital, Neijiang, Sichuan Province, China.
2Director, Laboratory of Human Anatomy, Southwest Medical University, Xianglin Road, Longmatan District, Luzhou City, Sichuan Province, China.
Kaiwen Yang
YangTel: 13340781717;
Email: 821575943@qq.com
Received : Oct 26, 2024 Accepted : Nov 12, 2024 Published : Nov 19, 2024 Archived : www.meddiscoveries.org
Background: Rheumatoid Arthritis (RA) primarily affects joints but can also impact the brain. Research suggests RA may alter brain function through inflammation, but the causal link remains unclear.
Method: This study utilizes Mendelian Randomization (MR) to explore the causal relationship between RA and various neuroimaging features. Data were obtained from the UK Biobank, which included multimodal brain imaging and genetic data, and the FinnGen project, which provided genetic data on RA patients and controls. Instrumental variables were selected based on genome-wide significance, and MR analysis was performed using the Inverse-Variance Weighted (IVW) method, supplemented by MR-Egger regression and MR-PRESSO to ensure robustness.
Results: Significant associations were identified between RA risk and specific neuroimaging markers. A larger area of the left inferior temporal sulcus (S-temporal-inf) was associated with a reduced risk of RA (OR = 0.7582, p< 0.0001), while increased thickness of the left BA3b region also correlated with a lower RA risk (OR=0.8522, p=0.0007). Conversely, increased thickness of the left middle frontal sulcus (S-front-middle) and higher amplitude of rfMRI node 12 were associated with an increased risk of RA.
Conclusion: This study reveals a causal link between RA and changes in brain regions related to cognitive and sensory processing. These findings shed light on RA’s pathophysiology and highlight potential targets for personalized treatment. Further research is needed to confirm these associations and their clinical implications.
Keywords: Rheumatoid Arthritis (RA); Neuroimaging; Mendelian Randomization (MR); Brain imaging; Inflammation and Cognitive Function.
Rheumatoid Arthritis (RA) is a chronic systemic autoimmune disease that primarily affects the joints but can also involve other organs and systems, including the Central Nervous System (CNS) [1,2]. Recent research has increasingly suggested that RA is not merely a joint-limited disease; its pathophysiological processes may also impact the brain through chronic inflammation and immune responses [3,4].
Observational studies have shown that RA patients often exhibit neuropsychiatric manifestations such as depression, cognitive impairment, and behavioral changes [5]. Additionally, RA patients are at an increased risk of early brain changes, independent of classic risk factors. It is recommended that brain MRI assessments be considered for new-onset cognitive impairment and/or depression in RA patients until more data is available [6]. Fatigue in RA is associated with functional and structural MRI changes in the brain. Newly discovered and replicated neuroimaging correlations provide a basis for future targeting and stratification of this critical patient priority [7-9]. A study found that in fatigue RA patients, after MRI assessment, the mean curvature of the left superior temporal sulcus was most strongly selected during the feature selection step, followed by the surface area of the right frontal pole and the left bank of the superior temporal sulcus [10]. These observational studies provide preliminary evidence of the association between RA and changes in brain structure and function, but causality has not yet been clearly established. The inevitable confounding factors in observational studies complicate the interpretation of this association. Therefore, there is an urgent need for a method that can control for confounding factors to determine the causal relationship between RA and changes in brain structure and function.
Mendelian Randomization (MR) is a statistical method that uses genetic variation as an instrumental variable to study the causal relationship between exposure factors and disease outcomes [11]. Since genetic variation is randomly assigned at birth and is not influenced by environmental factors, the MR method effectively avoids the confounding factors present in traditional observational studies, making it a powerful tool for validating causal relationships [12]. This study aims to explore the causal relationship between neuroimaging markers and RA using the MR approach, particularly the causal link between cognitive impairment and RA, thereby providing new insights into the pathophysiological mechanisms of RA.
Brain IDP data
The data used in this study were sourced from the UK Biobank project, which includes multimodal brain imaging data and genetic data from approximately 40,000 participants. Brain imaging phenotypes covered T1-weighted structural MRI, T2-weighted FLAIR MRI, diffusion MRI (dMRI), and resting-state functional MRI (rfMRI). After rigorous quality control, 34,298 samples of British white ancestry were retained for analysis. The final dataset included 3,929 existing IDPs with extensive quality control measures and 6 derived summary linkage features [13].
Rheumatoid arthritis data
This dataset was obtained from the FinnGen project, a large-scale Finnish biomedical research initiative that combines biobank samples with extensive health records. The FinnGen project aims to study the genetic factors and pathomechanisms of various diseases through the integration of genomic data and health information. The RA patient group consisted of 13,621 individuals, with a control group of 262,844, and the specific data download address is https://storage.googleapis.com/f inngen-public-data-r10/summary_stats/finngen_R10_M13_RHEUMA.gz.
Selection of instrumental variables
Effective Instrumental Variables (IVs) were selected based on three key assumptions:
The first assumption is that the instrumental variables (single nucleotide polymorphisms, SNPs) are significantly associated with the exposure, which in this case is Clonal Hematopoiesis (CH). Instrumental Variables (IVs) were identified using a genome-wide significance threshold (P-value of 5×10-8) to ensure a strong association with CH. Different thresholds were set for various exposures to ensure a sufficient number of SNPs. The second assumption is that the instrumental variables are independent of any confounders that might influence the outcome. SNPs with linkage disequilibrium (R2<0.001 and Kb<10,000) were excluded to maintain the independence and validity of the IVs. The third assumption is that the IVs are not directly associated with the outcome, which in this study is RA. To verify this, the PhenoScanner database (http://www.phenoscanner.medschl.cam.ac.uk/) was used to exclude SNPs significantly associated with confounders, thereby minimizing the impact of horizontal pleiotropy. IVs with an F-statistic above 10 were considered strong to avoid bias from weak IVs. Finally, GWAS data from the IDPs and RA datasets were harmonized and validated to ensure the reliability of the selected IVs.
Statistical analysis
Inverse-Variance Weighted (IVW) method is the primary MR analysis method. It calculates a weighted average of the effect estimates for each IV, with weights being the inverse variance of each estimate, assuming all IVs are valid and affect the outcome solely through the exposure. Supplementary methods include MR Egger, Weighted median, and simple mode. Sensitivity analyses include MR-Egger regression and MR-PRESSO. MR-Egger regression detects and adjusts for pleiotropy by estimating the intercept; a significant non-zero intercept suggests pleiotropy. MR-PRESSO (Mendelian Randomization Pleiotropy RESidual Sum and Outlier) is a method specifically designed to detect and correct for pleiotropy and identify outlier IVs, reducing pleiotropy bias by iteratively detecting and correcting outliers to improve result accuracy.
Heterogeneity tests using Cochran’s Q-test evaluate the heterogeneity of IV effect estimates. Significant heterogeneity suggests different IVs may have different effect mechanisms, warranting further investigation. Robustness analysis includes a Leave-One-Out analysis, where each IV is sequentially excluded to assess its impact on the overall effect estimate, ensuring result robustness.
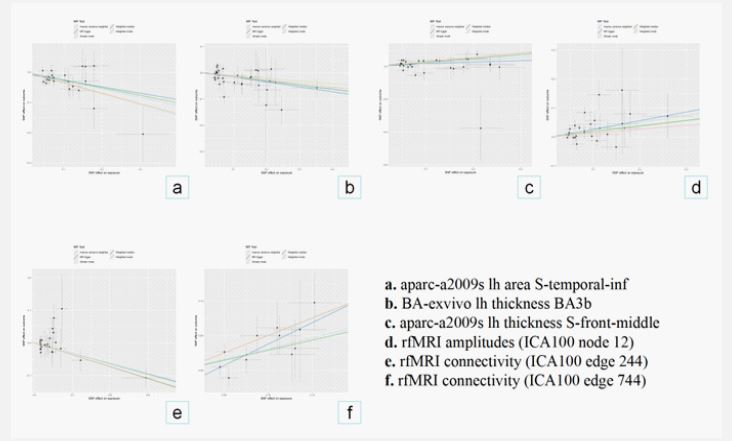
The relationship between the area of the left hemisphere’s inferior temporal sulcus (S-temporal-inf) and RA: OR=0.7582, 95% CI: 0.6751-0.8514, p< 0.0001, shows a significant association between larger S-temporal-inf area and reduced RA risk. The relationship between the thickness of the left hemisphere’s BA3b region and RA: OR=0.8522, 95% CI: 0.7768-0.9349, p=0.0007, indicates that greater BA3b thickness is associated with reduced RA risk. The relationship between the thickness of the left hemisphere’s middle frontal sulcus (S-front-middle) and RA: OR=0.0686, 95% CI: 0.2940-1.1987, p=0.0016, suggests that greater S-front-middle thickness may be associated with an increased risk of RA. The relationship between the amplitude of rfMRI node 12 and RA: OR=1.2835, 95% CI: 1.1212-1.4693, p=0.0003, indicates that greater amplitude of rfMRI node 12 is associated with an increased risk of RA. The relationship between rfMRI connectivity (ICA100 edge 244) and RA: OR=0.9001, 95% CI: 0.8541-0.9486, p< 0.0001, shows that increased rfMRI connectivity (ICA100 edge 244) is associated with reduced RA risk. The relationship between rfMRI connectivity (ICA100 edge 744) and RA: OR=1.3652, 95% CI: 1.1473-1.6246, p=0.0005, suggests that increased rfMRI connectivity (ICA100 edge 744) is significantly associated with increased RA risk, as shown in (Figures 2 and 3).


| Exposure | Outcome | Method | Heterogeneity | Pleiotropy | ||
|---|---|---|---|---|---|---|
| Q | Q_pval | Intercept | P | |||
| aparc-a2009s lh area S-temporal-inf | Rheumatoid arthritis | MR Egger | 19.3314 | 0.4358 | -0.005517 | 0.6277 |
| Inverse variance weighted | 19.5786 | 0.4845 | ||||
| PRESSO | 0.546 | |||||
| BA-exvivo lh thickness BA3b | Rheumatoid arthritis | MR Egger | 42.8393 | 0.0955 | 0.002816 | 0.6753 |
| Inverse variance weighted | 43.0786 | 0.1125 | ||||
| PRESSO | 0.167 | |||||
| aparc-a2009s lh thickness S-front-middle | Rheumatoid arthritis | MR Egger | 35.7212 | 0.0969 | 0.008087 | 0.3784 |
| Inverse variance weighted | 36.8246 | 0.0984 | ||||
| 0.132 | ||||||
| rfMRI amplitudes (ICA100 node 12) | Rheumatoid arthritis | MR Egger | 35.9669 | 0.0553 | -0.003731 | 0.7966 |
| Inverse variance weighted | 36.0686 | 0.0706 | ||||
| PRESSO | 0.095 | |||||
| rfMRI connectivity (ICA100 edge 244) | Rheumatoid arthritis | MR Egger | 19.7621 | 0.7592 | 0.000241 | 0.9591 |
| Inverse variance weighted | 19.7648 | 0.8026 | ||||
| PRESSO | 0.784 | |||||
| rfMRI connectivity (ICA100 edge 744) | Rheumatoid arthritis | MR Egger | 6.844 | 0.6534 | -0.023941 | 0.1784 |
| Inverse variance weighted | 8.9746 | 0.5345 | ||||
| PRESSO | 0.551 | |||||
These results suggest a significant causal relationship between certain neuroimaging features and rheumatoid arthritis, with the most notable associations being between changes in the S-temporal-inf area and rfMRI connectivity with RA risk.
Pleiotropy and heterogeneity analysis
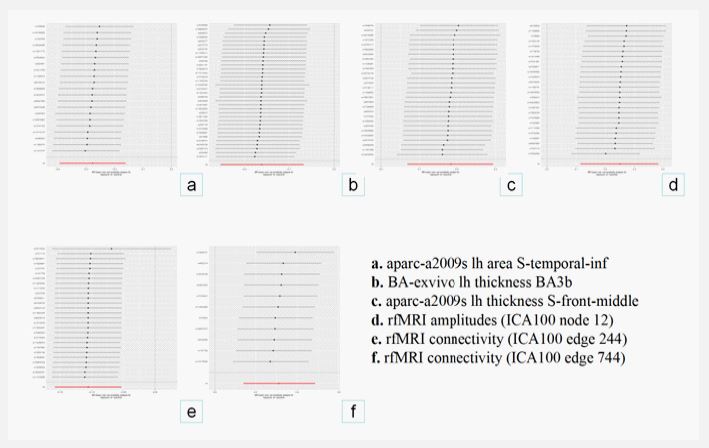
This study used multiple methods to test for pleiotropy and heterogeneity in the causal relationship between neuroimaging features and Rheumatoid Arthritis (RA). Overall, most features did not exhibit significant pleiotropy or heterogeneity, indicating that the MR analysis results were robust. All results did not show significant pleiotropy or heterogeneity, further supporting the credibility of the analysis. The overall results were robust (Table 1), and the Leave-One-Out analysis is shown in (Figure 4).
This study explores the causal relationship between various neuroimaging features and Rheumatoid Arthritis (RA) using Mendelian Randomization (MR), revealing significant associations between neuroimaging features and RA risk.
The relationship between the area of the left hemisphere’s inferior temporal sulcus (S-temporal-inf) and RA suggests that a larger area is significantly associated with reduced RA risk. The inferior temporal sulcus plays an important role in visual processing, semantic understanding, and object recognition [14]. The increase in the area of the inferior temporal sulcus may be associated with enhanced cognitive function, high-level semantic decoding, and integration of situational and visual memories [15,16]. Cognitive decline often accompanies the progression of RA, potentially involving cognitive tasks that integrate multimodal information and semantic understanding.
The thickness of the BA3b region is significantly associated with reduced RA risk, which may be related to altered sensory information processing in RA patients. BA3b is part of the primary somatosensory cortex and is responsible for processing tactile information from different parts of the body. Increased thickness may indicate enhanced sensory perception, potentially affecting chronic pain and inflammation in RA [17]. A thicker BA3b region may help process and regulate pain perception more effectively, thereby reducing the overall risk of RA or alleviating its symptoms [18,19]. Although persistent inflammation may lead to atrophy or dysfunction in certain brain regions, it may also trigger neural plasticity responses in other areas, enhancing their function. The increase in BA3b thickness may be part of this plasticity, helping to resist damage to sensory regions caused by inflammation [20-22]. This neural adaptation may be related to the regulation of neuroinflammation, which can be further explored using neuroimaging and neurobiological methods in future studies.
However, the increased thickness of the middle frontal sulcus (S-front-middle) suggests that changes in executive function and emotional regulation may play a detrimental role in the pathogenesis of RA. The middle frontal sulcus is located in the middle of the frontal lobe and is primarily involved in higher cognitive functions, including executive function, attention regulation, planning, decision-making, and emotional regulation [23,24]. The middle frontal sulcus, along with other regions of the prefrontal cortex, is involved in complex cognitive tasks and emotional processing [25]. The increased thickness of the middle frontal sulcus, which is closely related to higher-order cognitive function and emotional regulation, may reflect structural changes or functional overload due to inflammation and stress associated with RA. The increased prefrontal cortex thickness in RA patients may be related to neuroadaptive responses to chronic pain and inflammation stress and may also increase the risk of depression and anxiety [26,27]. Future research could further explore dynamic changes in the middle frontal sulcus in RA patients, particularly in long-term follow-up studies of emotional and cognitive function.
Understanding these structural changes in brain regions could provide new directions for personalized treatment strategies. Studies have shown that RA not only affects joints but also involves complex neurological changes closely related to chronic pain, mood disorders, and more. Neuromodulation techniques, such as Transcranial Magnetic Stimulation (TMS), can regulate activity in specific brain regions and alleviate sympsymptoms. For instance, TMS has been widely used in the treatment of depression, which is quite common in RA patients [28,29]. By modulating activity in brain regions such as the inferior temporal sulcus (S-temporal-inf) or middle frontal sulcus (S-front-middle), TMS may alleviate mood disorders and pain experiences in RA patients, thereby improving their quality of life. The impact of inflammatory mediators on brain structure and function has been confirmed in multiple studies, suggesting that reducing inflammation in specific cranial regions may alleviate emotional and cognitive disorders. These methods can significantly improve patients’ quality of life and slow the progression of RA.
Through these research directions, future efforts may develop more personalized treatment strategies, tailoring therapies to the specific neurological changes in RA patients, thereby significantly improving their quality of life. Further longitudinal and multimodal imaging studies will help comprehensively understand the impact of RA on the brain and drive improvements in treatment methods.
Funding: No funding.
Author’s contribution: KW and KWY participated in the design of the study. KWY performed the acquisition of data. KW and KWY performed the statistical analysis. DHX and KWY conceived of the study, participated in its design and coordination, and drafted the manuscript. KW revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Availability of data and material: All data generated or analysed during this study are included in this published article.
Ethics approval and consent to the participates: Not applicable.
Consent for publication: Not applicable.
Competing interests: The authors declare that they have no competing interests.
