Emergency Radiology Department, Ibn Sina University Hospital of Rabat, Rabat, Morocco.
Ibtissam El Oualic
Email: ibtissam.elouali94@gmail.com
Received : Oct 09, 2024 Accepted : Nov 06, 2024 Published : Nov 13, 2024 Archived : www.meddiscoveries.org
Penetrating Aortic Ulcer (PAU), first described in 1934, consists of an ulcerating atherosclerotic lesion located in the aortic wall that penetrates the intima and progresses through the internal elastic lamina into the media causing formation of hematoma within it. Ulcers of the aortic arch are less frequent and concomitant abdominal aortic aneurysm is a common finding in PAU patients. PAU can be discovered incidentally as well as it can be revealed by sudden-onset of thoracic or thoraco-abdominal pain. The disease becomes, then, a life-threatening emergency because of the high risk of aortic rupture, which is a rare but possible complication.
Computed tomography angiography is the diagnostic method of choice, demonstrating mural abnormalities and spatial relationships with adjacent structures. Magnetic resonance imaging allows unenhanced multiplanar imagining for patients with kidney failure. It is a better tool in differentiating acute intramural hematoma from atherosclerotic plaque and chronic intraluminal thrombus. It is not always easy to distinguish between the different entities of aortic disease in multiplanar imaging, the use of trans-esophageal-echocardiography, as a highly sensitive and specific method can be very helpful. We report the case of 78-year-old man who presented to the ER with an aggravation of progressive dyspnea, an acute abundant hemoptysis and rapid deglobalization.
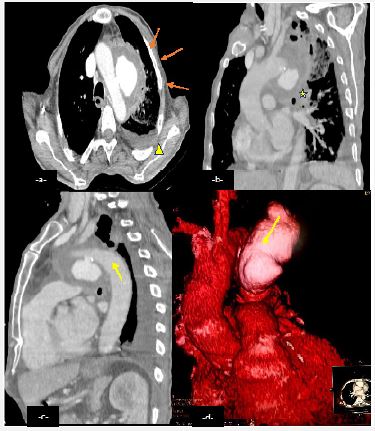
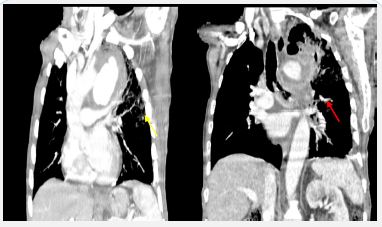
A CT angiography was performed in the radiology emergency department showing focal defect of an atherosclerotic aortic arch wall with contrast extravasation beyond intimal calcification, adjacent hematoma which extension led to the formation of a hyperattenuating huge smooth-walled sac (Figure 1). Compressing the left pulmonary artery and primary bronchi with hematic infiltration of the mediastinum, apical left parenchyma and left hemothorax (Figure 2) suggestive of an aortobronchial fistula considering the clinical symptomatology.
The patient was monitored and programmed for a thoracic endovascular aortic repair.
Usually, the PAU resolves completely or remain stable. But, in some cases, extensive hematoma causes stretching of the weakened aortic wall, leading to the formation of a saccular aortic aneurysm, aortic dissection or a false aneurysm with a high risk of spontaneous rupture especially when the thoracic descending aorta is involved. Current imaging modalities cannot reliably determine if an ulcer has penetrated the internal elastic lamina but some characteristic features may aid to diagnosis, like presence of intimal calcifications at the site of the defect, smooth interface with the intramural hematoma and contrast extension beyond intimal calcification.
This condition required a follow-up particularly during the 1st month after on-set. Symptomatic patients must be managed surgically in case of evidence of intramural hematoma expansion, signs of impending rupture, inability to control pain, or blood pressure changes. In cases of PAU localized to ascending aorta and/or arch urgent surgical management whether open surgical or Thoracic Endovascular Aortic Repair (TEVAR) is warranted. There is no uniform consensus as to when to choose between expectant and surgical management in cases of PAU localized to descending aorta. PAU complicated by sub adventitial aneurysm, presence of acute FID, enlarging IBPs, bronchial compression or aortobronchial fistula, and signs of distal embolization require urgent surgical management either open surgery or TEVAR.
PAU is commonly encountered beyond the sixth decade of life with male predominance Hypertension hyper lipidemia and diabetes are widely associated comorbidities, with current or past smoking Symptomatic clinical presentation is variable. PAU has a predilection for descending thoracic aorta and can be occasionally multiple. Prognosis of PAU depends on ulcer dimension and depth. The presence of pleural or pericardial fluid indicates imminent or frank rupture. Management in cases of thoracic aorta depends on the involved aortic segment.