Department of Medicine, University of Central Florida, USA.
Adishi Ranjan
Email: ad632190@ucf.edu
Received : Oct 08, 2024 Accepted : Nov 04, 2024 Published : Nov 11, 2024 Archived : www.meddiscoveries.org
Interstitial Cystitis (IC), also known as painful bladder syndrome, is a chronic disease that significantly reduces the quality of life for patients. Symptoms include pelvic pain, increased urinary frequency, urgency, and inflammation of the mucosa and interstitial layers of the bladder [1]. Etiology of IC is currently not fully understood and there are currently no uniformly established treatment strategies. Current experimentation studying biopsies of bladder epithelial cells from patients with IC reveals that changes in human bladder epithelial cell expression may be associated with the disease [2]. The changes in expression antiproliferative factor, interleukin-2, 4, 6, 8, tumor necrosis factor, nerve growth factor, insulin growth factor, transforming growth factor alpha, etc [2]. May be attributed to the cause of this disease as well. We hypothesize that inflammatory stress responses can result in these changes in gene expression and may stimulate a regulatory anti-inflammatory response to these changes.
The objective of this project is to identify the correlation between inflammatory response genes and Interstitial Cystitis through a comparative analysis of gene expression in IC and non-IC patients. This will elucidate the cause of IC and increase the effects of treatment by administering individualized and effective treatments. Although the etiology of Interstitial Cystitis is currently unknown, there have been a few hypotheses about the factors that contribute to the disease. Furthermore, these hypotheses include neurogenic inflammation, absorption of toxic substances, a deficient mucus layer or a leaky urothelium as potential causes for chronic inflammation [3].
The objective of this project is to identify the correlation between inflammatory response genes and Interstitial Cystitis through a comparative analysis of gene expression in IC and non-IC patients. This will elucidate the cause of IC and increase the effects of treatment by administering individualized and effective treatments. Although the etiology of Interstitial Cystitis is currently unknown, there have been a few hypotheses about the factors that contribute to the disease. Furthermore, these hypotheses include neurogenic inflammation, absorption of toxic substances, a deficient mucus layer or a leaky urothelium as potential causes for chronic inflammation [3].
Coincidently, all of these genes are up-regulated in IC patients indicating that a dominant feature of ulcerative IC is leukocyte invasion into the bladder. The gene ontology categories that are the most significant in this study include the up-regulation of responses to stimulus, defense responses, inflammatory responses and cell communication. The only processes that are downregulated include the transmembrane receptor protein serine/threonine kinase signaling pathway. Furthermore, the gene expression pattern in IC contains similarities to diseases of the immune system and lymphatic systems [4].
Gene Expression Omnibus is an NCBI tool that provides access to raw and processed data that can be used to study the expression of multiple genes. This tool will be used to analyze the raw data associated with the publication Gene expression profile of bladder tissue of patients with ulcerative interstitial cystitis [4]. This paper goes into cystoscopic and histological evidence for the cause of IC. First, a bladder sample is taken via cystoscopic examination from both IC and non IC patients. The IC patients are then split into nonulcerative versus ulcerative variations of IC, also known as Hunner’s Ulcer. This is done by taking two samples from the same patient, one from the tissue sample of the ulcer and one from non-ulcerative tissue. Patient homogeneity is extremely important when choosing patients for any clinical study. Therefore, all IC patients chosen for this study were all white females who had a bladder capacity of below 350 mL, nocturia, increased pain and greater urges for urination. Furthermore, the patients without IC had no symptoms of IC nor any Hunner’s Ulcers. All patients chosen for the study did not have any glomerulations or diverticulum. Lastly, the age and duration of symptoms were insignificant,t he same between the control and IC populations. Lastly, GeneChip Expression arrays were used to create a comparative analysis between the two groups [5].
The raw data obtained from each patient can be separated into the control group and IC group. For the purposes of this study, both ulcerative IC and non-ulcerative IC were grouped together because the paper shows no statistical significance that there are differences in gene expression between ulcerative and non-ulcerative IC patients. The six control patients are 203, 204. 212, 215, 216, 217 and the five IC patients, each of which had two sample, (non-ulcerative) and ulcus (ulcerative), and are 205, 206, 207, 208, 209, 210, 211, 213, 214, and 541. GEO2R provides a list of genes with their respective p-values, expression values for each gene for each patient and a probe ID for each gene [5].
(Figure 1) shows an example of a gene expression graph for serpin family A member 1 (SERPINA1), which had an extremely significant p-value. The expression values for the IC patients are much higher for this gene than for the patients without IC. After the raw data for each gene of interest was obtained, it was separated by patients into two groups, control and IC. Averages of these values and then a ratio of the averages were recorded. The percent standard deviation was calculated by dividing the standard deviation of each group by the average for that group. An average of these standard deviations were taken and then multiplied by the ratio of the average IC/Control to obtain the value for the error bars. These ratios and error bars are then graphed in order to compare the expressions between control and IC patients. The ratio of control genes, Tumor Necrosis Factor, Interleukin X, and actin, are also graphed for a comparison of expression values.

Lastly, a statistical analysis (Student’s T-test) will be used to determine statistical significance between the individual IC/Control ratios of genes of interest and those of ACTB, a control that has an average ratio of 1, which indicates no change in expression. P-values above the threshold of 0.05 indicate that the average IC/Control ratios show no change in expression.
Similarly, p-values below the threshold indicate changes in expression between the control (ACTB) and the gene of interest.
Upon further analysis, the following graph (Figure 2.1) depicts gene expression values of genes known to be markers of IC. The following genes are interleukin 3 receptor subunit alpha, RELT tumor necrosis factor, nerve growth factor, Insulin like growth factor , Prostaglandin D2 receptor, BTG antiproliferative factor 2, CXC motif chemokine ligand 6, CXC motif chemokine ligand 8, Vascular endothelial growth factor B, Prostaglandin Reductase 1, PERP (TP53 Apoptosis Effector), Epidermal Growth Factor Receptor and Heparin-binding EGF like growth factor. Like the graphs above, values significantly above 1 indicate expression values in IC patients are much higher than those in control patients with no IC. Similarly, values significantly below 1 indicate decreased expression in patients with IC. Noticeably, CXCL6 (CXC motif chemokine ligand 6) has increased expression in the patients with Interstitial Cystitis, indicated also by a ratio value of 16.744. PERP (TP53 Apoptosis Effector) has a value of 0.254, and therefore decreased expression in IC patients. The individual expression values are also depicted in (Figure 2.2) and (Figure 2.4). Along with this information, the p-values of both these genes are significantly less than the threshold value of 0.5, demonstrating that these genes are important biochemical markers in patients with IC and may give insight into the inflammatory pathways that result in the disease. It is worth noting that the bar for CXCL8 is not represented in (Figure 2.1), as it contains an outlier patient (GSM298211), which severely skews the ratio. The ratio value, 116, is therefore not represented in this Figure 2.

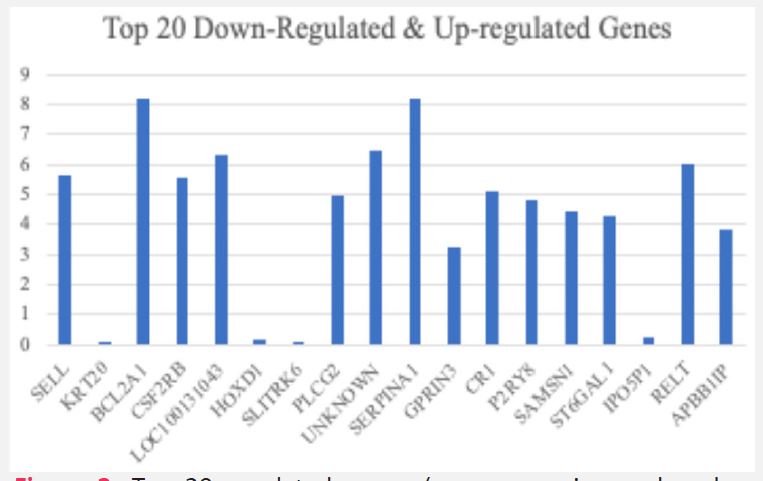
According to the initial study, immune system responses, cell communication, inflammatory responses and signal transduction are all upregulated in ulcerative interstitial cystitis patients, whereas, transmembrane receptor protein and the threonine kinase signaling pathway are down regulated. Figure 3 shows the top 20 genes downregulated and upregulated genes from this study, all of which have at least a 3-fold increase or decrease in expression. Of these top genes, L-selectin is found on leukocytes, BCL2 is a B-cell lymphoma that regulates apoptosis, and RELT TNF is capable of stimulating T-cell proliferation. The commonality between all genes is association with the immune system and immune response. This might explain why the gene expression profile of IC matches those of several immune system-related and lymphatic diseases.

Apoptotic proteins are those that trigger molecular events that eventually lead to cellular apoptosis. This is an important pathway in cells with infections as damaged synthetic machinery can cause disruptions to important cellular functions and eventually lead to more problems within the body. Cellular apoptosis of the bladder urothelium mediated by inflammation often occurs in patients with interstitial cystitis [6,7]. The upregulation of inflammatory signals like tumor necrosis factor alpha and p58 mitogen-activated protein kinase can lead to cellular apoptosis of urothelial cells. Upon further analysis, expression of the PERP TP53 Apoptosis Effector gene. PERP encodes a protein that plays an important role in epithelial development and tumor suppression and is regulated by p63. TP53 regulates several apoptosis pathways whose roles in p53-dependent apoptosis are still undetermined.
Overall, chemokines and cytokines (nerve growth factor and the family of interleukin genes) are responsible for inflammatory responses. Vascular endothelial growth factor and C-X-C chemokine ligands are also biomarkers of interstitial cystitis in patients and also pay a key role in the regulation of homeostasis [7,8]. CXCL10, which has a similar function to CXCL8 and CXCL6 play a crucial role in inhibiting angiogenesis, whereas, VEGF plays a stimulating role in angiogenesis. For this reason, in IC patients, an increase in the CXCL motif ligands and a decrease in the growth factor should be seen. This hypothesis is supported by (Figure 2.1) as VEGF has a ratio value of under 1, while the CXCL6 has a ratio over 1 (CXCL8 was omitted from the graph due to an outlier).
Another biochemical marker of interstitial cystitis is prostaglandin and the prostaglandin receptor family. They are synthesized from arachidonic acids via the cyclooxygenase pathway as a response to different pathopsychological stimuli. Furthermore, several naturally occurring prostaglandins are associated with inflammatory response and pain and fever management.
According to the evaluation of prostaglandin E2 and E-series prostaglandin receptor in patients with interstitial cystitis, there is an overproduction of PGE2 and associated receptor proteins in patients with IC as they play a significant role in the localized blockade action that may lead to relieving symptoms in IC patients. For this reason, the levels of prostaglandin and any related proteins will be elevated in diseased patients. According to (Figure 4.1), PTGDS (prostaglandin D2 receptor), the levels are very high in these patients. The raw data is further visualized in (Figure 3), where there is an apparent increase in levels of this protein. Contrastingly, according to the same (Figure 4), the levels of PTGR1 (prostaglandin reductase 1) are depressed in patients with IC. Prostaglandin involvement in the inflammatory pathway in IC patients shows the activation of prostaglandin and related protein. PTGR1 is involved in the inactivation of pro- and anti-inflammatory eicosanoids, and for this reason there must be a decrease in the amount of this protein, as prostaglandin plays an important role in the inflammatory response to IC [9]. The raw data for both of these proteins is depicted in (Figure 4). The juxtaposition of these two expression values show the increase of PTGDS and decrease of PTGR1 in patients with interstitial cystitis.
The analysis of gene expression in Interstitial Cystitis (IC) patients reveals key insights into the molecular mechanisms involved in this chronic inflammatory disease. The significant upregulation of certain genes and downregulation of others, particularly those involved in immune response, signal transduction, and inflammation, supports the hypothesis that IC is closely linked to dysregulated immune activity [10,11].
The overexpression of genes like CXCL6 (with a ratio of 16.744) underscores the prominent role of chemokines in driving inflammation. CXCL6, along with other CXC motif ligands, is known for its involvement in neutrophil recruitment and angiogenesis, and its increased expression suggests a heightened inflammatory response in the bladder tissue of IC patients [14]. Similarly, TNFSF14 and TNFSF13 (tumor necrosis factors) also show upregulation, which aligns with the observed increase in pro-apoptotic pathways in IC, leading to urothelial cell damage and bladder dysfunction [12].
On the other hand, the downregulation of PERP (TP53 Apoptosis Effector) with a ratio of 0.254 indicates a disruption in apoptosis pathways, which are crucial for cellular turnover and homeostasis. Given that PERP is regulated by p53 and plays a role in epithelial integrity, its reduced expression in IC patients might contribute to the characteristic loss of bladder urothelial integrity observed in the disease [12]. This finding may help explain the chronic and recurring nature of IC, as compromised epithelial barriers allow for persistent inflammation and tissue damage.
The involvement of prostaglandins in the pathophysiology of IC is further demonstrated by the elevated levels of PTGDS (prostaglandin D2 receptor), a marker of inflammation, and the downregulation of PTGR1 (prostaglandin reductase 1), a molecule involved in prostaglandin degradation [13]. The contrasting expression patterns of these two genes highlight the sustained inflammatory response in IC, wherein the accumulation of prostaglandins exacerbates bladder pain and discomfort.
Collectively, the findings align with the known association between IC and immune dysregulation, particularly in pathways involving apoptosis, chemokine signaling, and inflammation [10]. These insights are crucial for understanding the chronic nature of the disease and may offer potential therapeutic targets, such as chemokine inhibitors or drugs that modulate apoptotic pathways.
This study highlights the importance of examining gene expression profiles in interstitial cystitis patients to uncover the underlying mechanisms that contribute to disease progression. The upregulation of immune-related genes, including those involved in inflammation, chemokine signaling, and apoptosis, suggests that IC is driven by a complex interplay of immune dysregulation and chronic inflammation [11,14]. In particular, the significant overexpression of CXCL6 and underexpression of PERP point to key molecular drivers of the disease, which could be targeted in future therapeutic interventions.
Understanding the gene expression changes in IC not only advances our knowledge of the disease but also opens new avenues for developing more precise treatments. For example, targeting specific chemokines like CXCL6 or modulating apoptotic regulators such as PERP could help manage the inflammation and tissue damage seen in IC [10,13]. Moreover, the involvement of prostaglandin pathways suggests that anti-inflammatory drugs targeting prostaglandin receptors or synthesis may offer symptom relief.
Targeting CXCL6 in Interstitial Cystitis (IC) presents a promising avenue for more precise and effective treatment compared to the current symptom-focused therapies. CXCL6, a chemokine involved in recruiting immune cells, particularly neutrophils, plays a key role in promoting inflammation in IC. By directly targeting CXCL6, therapeutic strategies could block its interaction with receptors like CXCR1 and CXCR2, reducing the chronic inflammation in the bladder tissue [14]. One approach is the development of neutralizing antibodies that bind to CXCL6, preventing it from signaling and driving the immune response that exacerbates IC symptoms. Alternatively, small-molecule inhibitors could be designed to block CXCL6 signaling, offering a more targeted approach to modulating the disease’s inflammatory pathways.
In contrast to the specificity of targeting CXCL6, current IC treatments are primarily aimed at managing symptoms rather than addressing the underlying molecular drivers of the disease. The most commonly used therapies include oral medications like pentosan polysulfate sodium (Elmiron), which helps restore the bladder lining, and antihistamines like hydroxyzine, which reduce inflammation by blocking histamine release. Other treatments include Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) for pain management, antidepressants for alleviating chronic pain, and bladder instillations such as Dimethyl Sulfoxide (DMSO) and heparin, which are applied directly to the bladder to reduce pain and inflammation. While these treatments provide symptom relief for some patients, they often do not address the biological mechanisms driving the disease, leading to inconsistent efficacy and potential side effects [10].
Targeting CXCL6 offers several advantages over these conventional treatments. By focusing on the chemokine responsible for recruiting immune cells and promoting inflammation, gene-targeted therapies could directly reduce the chronic inflammainflammatory response in IC [14]. This approach contrasts with current treatments like NSAIDs, which have broad anti-inflammatory effects but do not specifically target the immune pathways central to IC. Additionally, by inhibiting CXCL6, it may be possible to prevent the urothelial damage caused by chronic inflammation, improving bladder function and reducing long-term symptoms. Gene-targeted therapies like CXCL6 inhibitors could also result in fewer systemic side effects compared to current treatments, which can cause gastrointestinal issues, sedation, or bleeding.
Moreover, targeting genes like CXCL6 could provide more durable and personalized treatment options for IC patients. Unlike existing therapies that mainly offer temporary symptom relief, gene-based treatments have the potential to modify the disease’s course by addressing its root causes. This precision allows for the development of personalized medicine, where treatment is tailored to a patient’s specific genetic profile. For instance, patients with high CXCL6 expression might benefit more from targeted therapies than those without such gene dysregulation [14].
Overall, targeting specific genes like CXCL6 represents a significant advancement in the treatment of IC, offering the potential for more effective, long-lasting, and personalized management of this chronic condition.
In conclusion, studying gene expression in interstitial cystitis is critical for identifying novel biomarkers and therapeutic targets, contributing to improved diagnosis, prognosis, and treatment of this debilitating condition [10]. It underscores the broader relevance of molecular research in unraveling complex disease mechanisms, ultimately paving the way for more effective and personalized treatments in the medical field.
