1Division of Hematology, Foundation IRCCS San Matteo, Pavia, Italy.
2Infectious Diseases Unit, Foundation IRCCS San Matteo, Pavia, Italy.
3Microbiology Unit, Foundation IRCCS San Matteo, Pavia, Italy.
4Department of Molecular Medicine, University of Pavia, Pavia, Italy.
Tobar Cabrera Claudia Patricia
Tel: +39-3494239522;
Email: claudiapatrici.tobarcabrera01@universitadipavia.it
Received : Jun 19, 2024 Accepted : Jul 29, 2024 Published : Aug 05, 2024 Archived : www.meddiscoveries.org
Breakthrough Fusarium infection during antifungal prophylaxis is an emerging problem and a life-threatening condition, especially in immunocompromised hematological patients; thus, early identification of infection and appropriate and aggressive antifungal therapy are required. Here, we present the first report on the combination therapy of high-dose Liposomal Amphotericin B (LAB) and Isavuconazole (ISA) successfully employed in a case of a 51-year-old woman with Acute Lymphoblastic Leukemia B (B-ALL) with disseminated Fusariosis while on Voriconazole (VRC) prophylaxis. The treatment obtained a clinical improvement until complete resolution with no signs of infection recurrence during the following 3 years.
Keywords: Liposomal amphotericin B; Voriconazole; Isavuconazole; Fusariosis; Leukemia.
Fusariosis is the second most common cause of disseminated fungal infection after Aspergillosis in patients with hematological malignancies; more often involving skin, lungs and paranasal sinuses [1]. A significant risk of morbidity and mortality in these patients has been reported, especially during chemotherapy-induced prolonged neutropenia or stem cell transplantation [1]. Moreover, the choice of the best treatment is a challenging issue; reliable laboratory tests on antifungal sensitivity are lacking, susceptibility to triazole antifungal agents is not predictable and no correlation between Minimum Inhibitory Concentrations (MICs) and outcome was observed [1]. For this reason, prophylactic anti-mold therapy is strongly recommended in these high-risk patients [2]. However, cases of breakthrough fungal infection during prophylaxis with VRC have been reported [2-4] leading to a rapid progression of the infection until death. Although LAB is considered the election therapy for invasive Fusariosis, its use as single agent showed unsatisfactory results owing to high rates of resistance. Therefore, higher doses of LAB or combination with VRC have been used in an attempt to overcome antifungal resistance [5]. Here, we describe a clinical case of disseminated Fusariosis arising during VRC prophylaxis, successfully treated with high-dose LAB and ISA without recurrence after further immunosuppression.
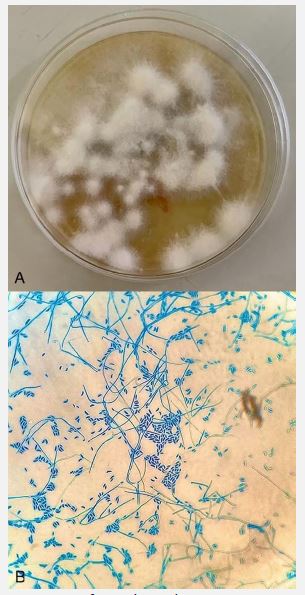
A 51-year-old female was diagnosed with a relapsed Philadelphia-negative B-ALL 17 years after the first diagnosis. In February 2021 she received re-induction intensive chemotherapy complicated by a fungal infection of the paranasal sinuses, classified as possible according to EORTC criteria [6]. The patient underwent surgical debridement of the nasal septum and an empirical treatment with VRC was promptly initiated leading to improvement and then resolution of the sinus infection. In March 2021 the patient received first consolidation with Idarubicin, Cyclophosphamide, Dexamethasone and Cytarabine and continued with VRC as secondary fungal prophylaxis. Ten days after the beginning of the chemotherapy, the patient developed febrile neutropenia, crampy pain to the lower limbs and muscular weakness associated with gait difficulties. In the meantime, painful subcutaneous nodules in the extremities, in the occipital region, at the trunk and at the left shoulder appeared (day 0). The nodules were initially homogeneous, erythematosus and well delimited, not necrotic or purulent (Figure 1A). A lower limb venous doppler ultrasound, the microbiological and cytofluorimetric analysis on cerebrospinal fluid, echocardiography, and serologic assessments testing Borrelia burgdorferi, Bartonella henselae and Cryptococcus antigen were all negative. Blood culture tests revealed Pseudomonas aeruginosa, therefore antibiotic therapy with ceftazidime and meropenem was performed. Owing to persistent fever and worsening of cutaneous lesions tedizolid was added to the antimicrobial therapy, without benefit. On day +7 Computed Tomography (CT) chest scan showed a pseudo nodular consolidation with irregular delimitation located in the medial segment of the inferior left lobe, suggestive of opportunistic infection. Bronchoscopy, brain and abdomen CT scan, explorative lumbar puncture and fundus oculi examination, resulted all negative. On the same day the patient underwent skin lesions biopsy and empirically started LAB at dose of 3 mg/kg, while VRC was discontinued. Morphological pattern of the skin lesion showed a dermal lymphocyte, granulocyte infiltration with perivascular distribution and areas of steato-necrosis in the hypodermis. PAS and Gomori-Grocott histochemical stains did not detect the presence of fungi, while culture of the skin swab and skin biopsy were indicative of Fusarium genus (Figure 2A-B).
Patient was therefore diagnosed with disseminated Fusariosis due to multiple painful metastatic skin lesions and likely lung involvement, accordingly antibiotic treatment was discontinued. On day +17, due to the persistence of cutaneous lesions and fever LAB was increased to 5 mg/kg and oral ISA at 200 mg/die was added in the attempt to better overcome any possible resistance. This combination therapy achieved stable apyrexia after 24 hours. On day +24, after 7 days since the start of the combination of high-dose LAB and ISA, the nodules gradually improved, becoming less numerous, sized-reduced, less erythematous and not painful (Figure 1B). After further twenty days, chest CT scan showed a dimensional reduction of the pulmonary nodule, a necrotic and a minimal ground glass component. On the other side, the skin lesions became dyschromic, flat and almost completely resolved. Due to renal toxicity, we decided to discontinue LAB after a total dose of 7400 mg and to continue anti- fungal therapy with ISA as single agent.
The patient received the third consolidation cycle with high doses of methotrexate and cytarabine and after that, due to the persistence of measurable residual disease, she was switched to monoclonal anti-CD22 antibody, Inotuzumab-Ozogamicin, as bridge to allogeneic stem cell transplantation, obtaining deep molecular response at the time of the transplant. Chest CT scan before transplant was negative and only dyschromic skin changes on lower limbs were present. ISA was maintained throughout the whole peri-transplant period. 3 years after the onset of skin lesions and 30 months after allogeneic transplant, the patient is in good general condition, without any signs or symptoms of recurrence of the infectious disease (Figure 1C).

Fusarium species are hyaline filamentous fungi widely distributed in soil, plant debris, air and water [1,7]. The mainly entry routes are airways, through damaged mucous membranes or skin and nails injuries [1]. Most frequently species causing infection in humans are Fusarium Solani (50%), Fusarium Oxysporum (20%) and Fusarium Verticillioides (10%) [4]. Patients affected by acute leukemia and those who undergo bone marrow transplantation carry the highest risk to develop disseminated Fusariosis due to prolonged neutropenia and cellular secondary immunodeficiency related to aggressive and chronic immunosuppressive therapies [1].
Skin lesions are the most common clinical manifestation [8], appearing in about 70% of cases, are often the only sign of disease and frequently appeared as painful, purulent and necrotic nodules [9]. The muscle involvement is quite rare and has been described in 15% of cases [7]. Lung involvement is frequent in immunocompromised patients. Our patient presented disseminated involvement of the skin, the muscles and the lung with painful subcutaneous nodules lacking the typical necrotic and purulent aspect [8,9] associated with myalgias and gait difficulty; the pulmonary localization, was attributed to Fusarium spp. due to the concomitant appearance with skin lesions and to the optimal response to the antifungal treatment.
Given the aggressiveness and the rapidity of infectious dissemination, a prophylactic anti-mold treatment is recommended in high-risk patients [2]. However, breakthrough Fusarium infections during prophylactic antifungal therapy have been described and represent a challenging issue [2], associated with high mortality rates, since Fusarium spp. have shown intrinsic resistance to antifungal agents [1]. Also in our case prophylactic VRC failed even if continuing monitored drug plasma levels were adequate. Recent studies have reported several cases of breakthrough fungal infection during VRC [2,3], possibly related to immunological host factors, intrinsic resistance of pathogens against the molecule or low bioavailability of the drug at the infection site [4,10]. In vitro antifungal susceptibility tests have shown that some Fusarium spp. exhibit high MICs for agents such as VRC and LAB [9,11], however, VRC or LAB monotherapy often obtain modest results [12], since no correlation between MICs and clinical outcome was reported [1]. The choice of a combination therapy between a broad-spectrum antifungal agent with a high bioavailability as ISA [13] with high doses of LAB to reach all possible sites of infection had the aim to adequately and rapidly face a such severe life-threatening complication; ISA could be effective in a wide range of rare invasive fungal diseases, including those caused by Fusarium spp. and in vitro shows the ability to inhibit Fusarium spp. growth [13,14]. In addition, low toxicity profile has been reported with ISA compared to VRC [14] making it an attractive drug for combination treatment. Our approach allowed us to obtain consistent lesions improvement both in the skin and in the lung and to continue the treatment for a long time with ISA monotherapy to contain the toxic effect by high doses of LAB and to prevent possible recurrence during following immunosuppression.
This report shows that diagnosis of Fusarium infection requires a highly clinical suspicion since clinical picture may not be as usual as described in the literature. To the best of our knowledge, this is the first report on the combination therapy of ISA and LAB successfully employed in a case of disseminated Fusariosis while on triazole prophylaxis; we provide a valid therapeutic option that may be an effective and safe therapeutic strategy for this severe infection in immunocompromised patients. Better outcome is associated with a prompt effective treatment; therefore, physicians should consider to rapidly start this combined antifungal treatment when Fusariosis has been diagnosed.
Funding disclosure: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest: The authors declare that they have no conflict of interest.
Author contributions: Conceptualization, supervision, validation, review and editing: ZP, AL; Writing-review, editing, data curation and analysis: TCCP and CC; review-editing, data curation and analysis: TCCP, CC, GE, MG, CL, BE, SR, GM,ZP, RE, RM, DA; Resources: CC.
