Cardiology Department, CHU Ibn Rochd, Casablanca, Morocco.
A El Bouazizi & R Habbal
Email: asmaaelbouazizi@gmail.com
Received : Jun 22, 2024 Accepted : Jul 17, 2024 Published : Jul 24, 2024 Archived : www.meddiscoveries.org
Dilated cardiomyopathy is a heart condition characterized by the dilation of heart chambers and decreased systolic function of the left ventricle. Hyperthyroidism, an excessive secretion of thyroid hormones, can induce severe cardiovascular disturbances, including dilated cardiomyopathy. This case report documents a 60-year-old man presenting with severe dilated cardiomyopathy secondary to hyperthyroidism, leading to a rapid fatal outcome despite adequate medical management. The complications and severity of the condition highlight the necessity for prompt recognition and intervention.
Dilated Cardiomyopathy (DCM) is characterized by the dilation of heart chambers and decreased systolic function of the left ventricle. The European Society of Cardiology (ESC) criteria define DCM by left ventricular dilation and systolic dysfunction not explained by abnormal loading conditions or obstructive coronary artery disease [1]. Etiologies include coronary artery disease, viral infections, toxins, and endocrine disorders such as hyperthyroidism. Hyperthyroidism, a pathological state where the thyroid gland produces an excessive number of thyroid hormones, can cause severe cardiovascular disturbances [2,3]. This case report illustrates an example of severe DCM secondary to hyperthyroidism, with a fatal outcome despite prompt management.
A 60-year-old man, a chronic smoker without significant medical history, was admitted to the emergency department with progressively worsening dyspnea over two weeks. Symptoms included progressive lower limb edema and frequent diarrhea (approximately seven stools per day). The patient reported progressive fatigue and a notable decrease in his usual physical activity.
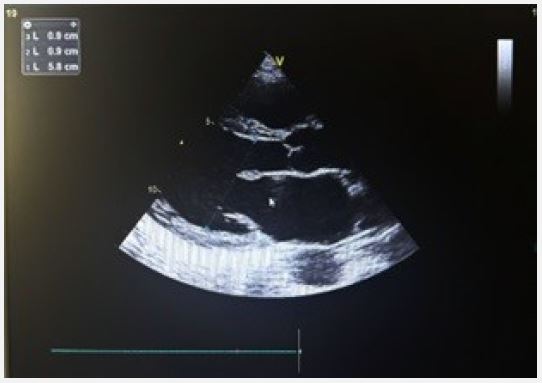
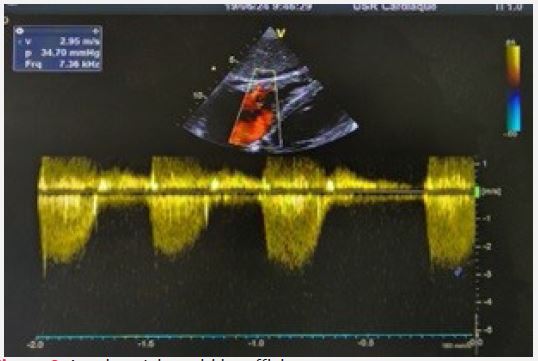
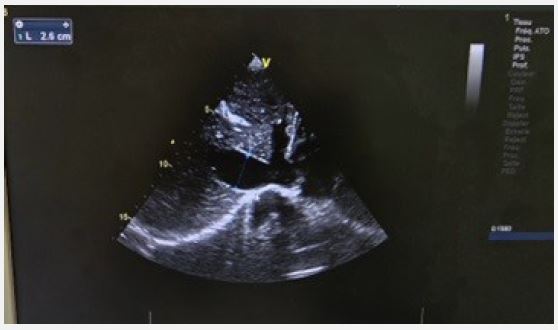
On clinical examination, the patient had dyspnea at rest, a blood pressure of 120/80 mmHg, and obvious exophthalmos. The Electrocardiogram (ECG) showed atrial fibrillation with a rapid ventricular rate of 108 beats per minute. Transthoracic echocardiography revealed dilated cardiomyopathy with global hypokinesis, a reduced Left Ventricular Ejection Fraction (LVEF) of 15%, left atrial dilation without intracavitary thrombus, moderate mitral regurgitation, and severe tricuspid regurgitation with an estimated Pulmonary Arterial Systolic Pressure (PASP) of 70 mmHg. The right ventricle was dilated but with preserved systolic function, and the Inferior Vena Cava (IVC) was dilated and non-compliant. A circumferential pericardial effusion without signs of tamponade was also present.
Biological tests showed a Thyroid-Stimulating Hormone (TSH) level below 0.01 mIU/L, Free T3 (FT3) at 21.9 pg/ml, and Free T4 (FT4) at 63 pg/ml, confirming severe hyperthyroidism. Other biological parameters, including electrolytes, liver enzymes, and renal functions, were within normal limits. Coronary angiography revealed normal coronary arteries, excluding obstructive coronary artery disease.
The patient was initially treated with intravenous furosemide, potassium supplementation, therapeutic anticoagulation with heparin, and the introduction of carbimazole at 80 mg/day to control hyperthyroidism. Despite this management, the patient’s clinical condition rapidly deteriorated. He developed refractory heart failure with severe hypotension and anuria. Despite resuscitation measures, the patient was declared deceased after 24 hours of hospitalization.

Dilated cardiomyopathy associated with hyperthyroidism, although rare, has severe implications for cardiac function. An excess of thyroid hormones causes an increase in basal metabolism and volume overload on the heart, leading to chamber dilation, decreased myocardial contractility, and arrhythmias such as atrial fibrillation [4,5]. Pathophysiological mechanisms include increased cardiac output, reduced peripheral vascular resistance, and positive inotropic and chronotropic effects on the heart [6,7].
Clinical manifestations of hyperthyroid heart disease include tachycardia, atrial fibrillation, left ventricular hypertrophy, and dilated cardiomyopathy. Chamber dilation can lead to functional valvular insufficiency, as observed in this case with mitral and tricuspid regurgitation. The high pulmonary arterial pressure observed is also common due to high cardiac output and increased venous pressure [8].
Case studies, such as that of Watanabe et al. (1995) [4], show that even with the normalization of thyroid function, cardiac dysfunction may persist, necessitating the use of beta-blockers to improve clinical symptoms. Chariyawong et al. (2019) [5] highlight the importance of early detection and management to restore cardiac function. Bassilly et al. (2019) [6] mention that pulmonary hypertension can contribute to isolated right heart failure in thyrotoxic patients. Finally, Bauerlein et al. (1992) [7] discuss the possibility of reversible dilated cardiomyopathy with appropriate treatment of thyrotoxicosis.
Management of these patients requires a multidisciplinary approach, including control of thyrotoxicosis with antithyroid drugs, beta-blockers to control heart rate, and diuretics to manage volume overload. Managing cardiac complications, such as atrial fibrillation, is essential to prevent thromboembolic events. In severe cases, more aggressive interventions, such as plasmapheresis or thyroid surgery, may be necessary [8,9].
Despite prompt and appropriate management, some patients may rapidly deteriorate due to the severity of cardiopathy and associated complications. Studies have shown high mortality in patients with severe hyperthyroidism and dilated cardiomyopathy, especially in the presence of complications like atrial fibrillation and acute heart failure [10].
This case highlights the severity of dilated cardiomyopathy associated with hyperthyroidism and the need for rapid recognition and aggressive medical intervention. Despite appropriate therapeutic interventions, the prognosis remains poor in severe forms. Further research is needed to better understand the underlying pathophysiological mechanisms and optimize treatment strategies for these high-risk patients.
