1Immunohematology and Transfusion Medicine, “San Luca” Hospital, Vallo Della Lucania, Italy.
2Nephrology Unit, “SS. Maria Addolorata” Hospital, Eboli, Italy.
Giovanni D’Arena
Email: g.darena@aslsalerno.it
Received : Jan 19, 2024 Accepted : Feb 16, 2024 Published : Feb 23, 2024 Archived : www.meddiscoveries.org
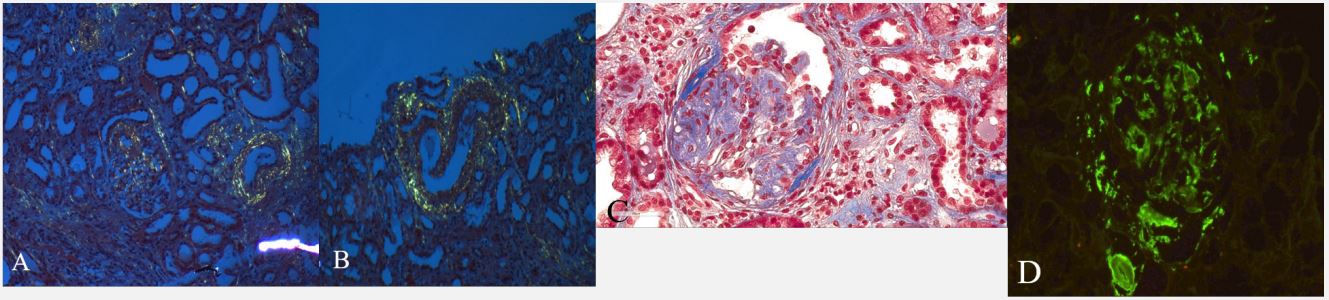
The association between monoclonal gammopathies and kidney damage is commonly seen. In Multiple Myeloma (MM) the renal involvement is a sign of active disease to be treated. In addition, a clinical condition called “monoclonal gammopathy of renal significance” has been proposed in 2012 to describe hematological conditions producing a monoclonal immunoglobulin associated with kidney injury outside of MM and Monoclonal Gammopathy of Undetermined Significance (MGUS). A 45 year-old male with IgG/Kappa MGUS followed since October 2011 underwent to a renal biopsy because of proteinuria without clear evidence of overt evolution in MM at lab tests (December 2015). The biopsy showed a kidney involvement as detailed in Figure 1 and patient started induction therapy with carlfizomib, cyclophosphamide, and lenalidomide (KCD regimen) for 4 cycles and autologous stem cell transplantation (October 2016) followed by maintenance therapy with carfilzomib, dexamethasone, and lenalidomide (KRD) for 2 years. Since December 2015 only lenalidomide is currently given. The patient is alive in very good clinical and laboratory remission at +94 months from the start of therapy. This case clearly shows that a renal biopsy needs to be performed when an alteration of urine analysis or an impairment of renal function is seen during the course of monoclonal gammopathies due to the great relevance in the assessment of clinical risk and in therapeutic approach to these diseases also when apparently both clinical and laboratory findings are not suggestive of disease progression.