1Water and Land Resource Centre, Addis Ababa University, P. O. Box 7985, Addis Ababa.
2Ethiopian Public Health Institute, Addis Ababa, P. O. Box. 1242, Addis Ababa..
Hailu Shifarew
Email: Hailu2nd@gmail.com & Hailushi31@yahoo.com
Received : Aug 12, 2023 Accepted : Sep 05, 2023 Published : Sep 12, 2023 Archived : www.meddiscoveries.org
Background: Seeing difficulties like blindness and partial blindness are affected by a number of intrinsic and extrinsic factors. The objective of this study is to evaluate whether seeing difficulties are associated with extrinsic (external) factors like environmental, educational, and socioeconomic status of people.
Methods: After checking the plausibility of the data, a multiple linear regression model was run and revealed some external factors affecting both blindness and partial blindness.
Results: Our study results indicate that blindness was significantly affected by different environmental and socio-economic factors like use of energy use (cow dung for cooking), access to information (no radio), and lack of sanitary services (including use of unprotected well water for drinking and washing purposes, lack of toilet facility, waste disposal inside the compound, burning in the compound and public disposal of wastes). Similarly, partial blindness was significantly affected by a number of factors such as poor economic conditions of the household (e.g. houses made from mud floor, wood, and mud wall), usage of energy use (cow dung for cooking), lack of information source (e.g. radio and telephone), usage of unprotected well water for drinking and washing hands and faces, the use of river water for drinking and washing purposes, and lack of education. Furthermore, because 94% of the population of the region lived more than 15 km away from the hospital, 33% were far from clinics, and 34% were more far from health centers, access to health services had a significant impact on both blindness and partial blindness.
Conclusion: These all show that people who lived in such remote places had poor access to medical facilities. It also has an impact on the ability to prevent and treat various diseases as well as the ability to see problems.
Keywords: Amhara region; Blindness; Hygiene and sanitation; Partial blindness; Seeing difficulty; Trachoma.
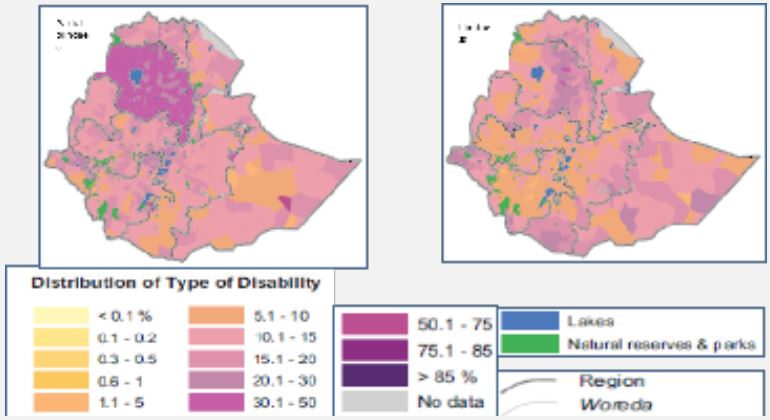
More than 80,000 persons were registered as disabled people in Ethiopia, which has a large number of people with various sorts of disabilities (CSA-IFPRI, 2010). Lower limb disabilities (19.9), seeing difficulties (19.2), full blindness (11.7), hearing difficulty (9.1), and upper limb disabilities (7.5) were among the most prevalent disability kinds by percentage recorded. From these statistics, it can be inferred that 30.9% of impaired people had vision problems, including both partial and total blindness. Even though the majority of these handicap kinds were reported across the nation, the Amhara area had a disproportionately high rate of vision impairment and total blindness. About 33 woredas/districts in the Amhara region were severely impacted by full and partial blindness, and one woreda in the Somali region had a full and partial blindness rate of over 20% relative to the impaired population in that woreda. In several woredas across the nation, full blindness was also an issue (Figure 1).
According to reports, trachoma is one of the main causes of low vision and blindness, and about 80% of blindness in Ethiopia is thought to be avoidable (can be treated), i.e., either preventable or curable [1]. The prevalence of trachoma, including trachomatous trichiasis and active trachoma, is concentrated in a few areas of the nation (Amhara: 63%; Oromia: 41%; Southern Nations and Nationalities and Peoples Region-SNNPR: 33%), which together make up a sizable portion of the population of the nation [1]. According to Ethiopia’s official census on trachoma prevalence from 2007, 40% of children aged 1 to 9 had active trachoma. Amhara area had the highest rates of trichiasis in people aged 15 and older (5%) and active trachoma in children aged 1 to 9 (63%)
The Amhara region has a high rate of disability according to the census, which prompted researchers to look into the matter further by taking into account several explanatory factors that were presented with the instances in various case studies. The main objective of this paper is to assess the risk factors for Amhara Region, Ethiopia’s partial and total blindness, which is one of the disabilities, using spatial and regression analyses.
This analysis included data from various sources. The Central Statistical Agency’s (CSA) 2007 [2] Population and Housing Census of Ethiopia was one of the primary sources. Other datasets used in this research included those from the Demographic Health Survey (DHS, 2010) and Welfare Monitoring (2011) [3-12].
Multiple Linear Regression was chosen as the statistical method for the investigation after considering its plausibility. Because manually estimating the coefficients of multiple linear regression was laborious and time-consuming, we used the statistical program SPSS 20.0 to analyze the data. Additionally, mapping of these potential risk variables was made available for display using free software (QGIS 3.8).
Multiple linear regression
The following general characteristics were taken into consideration as potential underlined (direct) and indirect factors (related factors) for evaluating such health issues (disability typ
• Education or access to information
(illiterate, not having a radio, not having
TV),
• Access to health facilities (hospitals, health
centers, and clinics),
• Infrastructure access (water access, road
access and service quarters like market and
information by closeness or remoteness),
• Economic factors (material types and qualities
used for housing construction such as mud floor
or wood mud wall and thatch roof),
• Energy use like cooking fuel types such as cow
dung, firewood or other clean energy,
• Environmental health and sanitation (water
sources and availability like an open lake or
river source, toilet facility, health facility,
waste disposal systems like disposal to open
space or dump to nearby areas).
However, rather than measuring these general parameters directly, their particular features were used instead. Economic considerations, such as the materials used to build homes, were assessed, and environmental health considerations, such as the sources of drinking and washing water, were also monitored and analyzed.
The response y may be related to k regressors or predictor variables (multiple linear regression model) as given in Equation 1 using “enter” method in SPSS.
Y = β0 + β1 X1 + β2 X2 +....... +βk Xk+ ε ........(1)
Where, β0, β1, β2........ β k are the coefficients of multiple regression; and ε is the error term distributed normally and independently with constant variance. The parameter represents the expected change in the response y per unit change in xi when all of the remaining regressor variables xi are held constant.
Estimation of model parameters
The coefficients are estimated by applying Least-squares methods by minimizing the sum of squares of residuals.
The model assumptions: Consider n observations (n > k), model assumptions were tested such as:
i) The error term ε , E (ε ) = 0 and Var(ε ) = 2
σ constant variance
ii) The errors are uncorrelated.
iii) The regressed variables, x1,
---, xk are fixed.
iv) Multicollinearity among different risk
factors, and
v) Normality tests were carried out before data
interpretation.
Then the regression equation by considering the significant variable was given in Equation 2. If we formulate a multiple regression model for these significant variables,

Where, β0 ,− − −,β7 are the model parameters; and ε is the error term distributed normally and independently with constant variance.
The representation of variables is denoted as follows:
| X1--- cow dung for fuel | X5--- waste disposal: dumped inside the compound |
| X2--- households do not have radio | |
| X3--- water source: unprotected well | X6--- waste burned in compound |
| X4--- household no toilet facility | X7--- public dumping of waste |
The estimated model equation 2 was replaced by their respective coefficients (Equation 3).

Now, the formula for the linear multiple regression is given in Equation 3. Let Y- the response variable represent the partial blindness model:

Thus, using the variance inflation factor (VIF) test, auto-correlated components were discovered and eliminated from the analysis. Values of VIF greater than 10 were taken into consideration to remove a variable from the analysis. The following nine independent factors were kept in the study in place of the weakly correlated independent variables from the associated independent variables, including:
| X1--- mud floor | X6---- use of river or pond water for drinking |
| X2--- wood and mud wall | X7---- no regular education or schooling |
| X3--- cow dung cake for fuel | X8---- has no toilet facility |
| X4--- has no radio | X9---- wastes dumped inside the compound |
| X5--- unprotected water drink-ing water |
Where, β0 , − − − β9 are model parameters estimated by least square methods;ε is the error term assumed normally and independently distributed.
The estimated equation was replaced by coefficients of predictor variables was given in Equation 5:

The variables (X1, X3, X4, X7, and X9) had a positive effect on partial blindness whereas the variables (X2, X5, X6, and X8) had negative effects on partial blindness due to the negative regression coefficients. Additionally, X4's contribution to the model is less encouraging because it had a coefficient that was nearly zero. Before stating that these characteristics have a negative impact on partial blindness, they should be carefully evaluated.
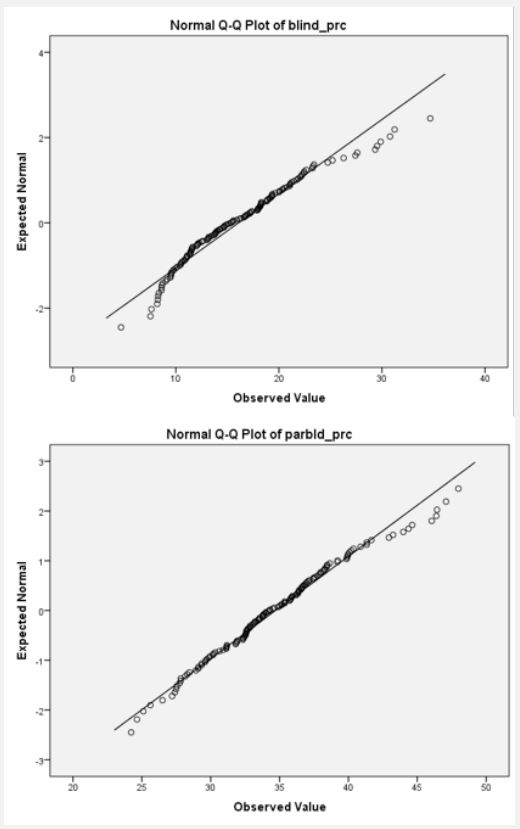
Prior to continuing with the regression analysis, we had to ensure that the dependent variables (blindness and partial blindness) were normal (Figure 2). The outcome was shown in Annex 1. Due to the fact that the blindness and partial blindness tests for normality had large p-values (P-values of 0.099 and 0.2, respectively), the results were not far from normal. Since we had a high sample size of more than 2000 instances, the Kolmogorov-Smirnov test was preferred over the ShapiroWilk's test. As a result, the data for both variables had a roughly normal distribution.
Blindness
Following the findings of the aforementioned exploratory activity, blindness was considered for multiple linear regression, with the following predictor variables: public dump (dumping waste in public), lack of telephone, wood and mud floor (materials used to build walls), roof-thatch (materials used to build roofs), mud floor, cow dung (used as fuel for cooking), water source (unprotected well, river/pond), waste disposal (dumped inside the compound and open space disposal), and burned (wastes), lack of toilet facility, lack of attendance at school, lack of radio, and lack of TV as the predictor variables.
Several variables were kept in the study based on the multiple linear regression and their contribution to the model. Seven of these factors (cow dung, has no radio, unprotected well, no toilet facility, wastes thrown inside the compound, wastes burned inside the compound, and public waste dumping) had statistically significant p-values of less than 5% and were thus considered statistically significant (Table 1).
Eight more factors that were not statistically significant included having a mud floor, a thatch roof, a wood and mud wall, not attending school, having no phone or TV, getting water from a river or pond, and disposing of garbage in an open area. The multiple regression model, however, is significant overall with a p-value of 0.001 and a high F-value of 13.745 (Annex 2).
|
Model variables (variables in percent) |
Unstandardized coefficients | Standardized coefficients | T | Sig. | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| (Constant) | 5.03 | 2.316 | 2.17 | 0.03*** | |
| Mud floor | 0.01 | 0.035 | 0.03 | 0.38 | 0.71 |
| Thatch | 0.01 | 0.011 | 0.02 | 0.33 | 0.74 |
| Wood/mud wall | -0.01 | 0.021 | -0.02 | -0.48 | 0.63 |
| Cow dung | 0.03 | 0.008 | 0.17 | 4.05 | 0.001*** |
| No attended(no schooling) | 0.02 | 0.020 | 0.07 | 1.05 | 0.29 |
| Has no radio | 0.001 | 0.001 | 0.83 | 6.67 | 0.001*** |
| Has no telephone | 0.001 | 0.001 | -0.75 | -1.34 | 0.181 |
| Has no TV | 0.001 | 0.001 | -0.22 | -0.38 | 0.71 |
| Unprotected well | -0.062 | 0.019 | -0.17 | -3.28 | 0.001*** |
| River/pond | 0.005 | 0.016 | 0.02 | 0.34 | 0.732 |
| No toilet facility | 0.054 | 0.014 | 0.23 | 3.85 | 0.001*** |
| Open space disposal | 0.014 | 0.032 | 0.05 | 0.43 | 0.67 |
| Dumped inside compound | 0.001 | 0.001 | 0.19 | 3.33 | 0.001*** |
| Burned inside compound | 0.001 | 0.001 | 0.18 | 2.55 | 0.011*** |
| Public dump | 0.097 | 0.033 | 0.17 | 2.96 | 0.003*** |
| *** significant at P<0.05 | |||||
With the exception of X3 (unprotected well), all significant variable coefficients are positive and have a favorable impact on blindness. That implies if more people are using uncovered wells for their everyday water needs (drinking and washing), it leads to more serious sanitary issues and an increase in blindness, as represented by trachoma. Additionally, the coefficient of X6 (wastes burned inside the compound) requires more decimal places because it is not exactly zero.
Variables including cow dung, no radio, no toilets, burning garbage, and public waste dumping had a favorable impact on blindness. This implied that blindness in the area could be reduced if these problems could be treated effectively. Because adjusted R-square penalizes the needless increment of the coefficient of determination (R-square) for more than two predictor variables, it was preferable to R-square in multiple linear regression.
Taking into account the model summary (Annex 3), the modified R-square is 0.313, demonstrating the model's capability for explanation. The response variable for blindness is explained by the explanatory variables in 31.3% of the model.
According to this findings, factors including the use of cow dung as fuel for cooking, the absence of a radio, a bathroom, burned waste, and open trash disposal increases the risk of blindness.
After standardized the regressed variables, the beta coefficients of the variables were changed once the regressed variables had been normalized. "has no radio" made a significant positive impact on blindness. About 0.832 units are contributed by this variable for every unit change in blindness. This contradicts the initial hypothesis that access to radio or other information sources may improve health status, even though this is not the case for this variable. On the other hand, those without access to a telephone experienced these health issues. Accordingly, there were roughly 0.75 units of negative contributions to blindness for every unit of change in blindness, which suggested that "having a telephone" may reduce blindness by up to 75%. As a result, those who owned a phone were more aware of and concerned about their health (Table 1).
Partial blindness
Predictor variables for partial blindness in multiple regressions were comparable to those for blindness. These factors included wastes that were burned inside the compound, no telephone, a public dump, a wood or mud wall, irregular schooling, dumping waste into rivers or ponds, cow dung, thatch roofs, unprotected wells, dumped inside the compound, no toilet facility, mud floors, no attended schooling, wastes that were burned inside the compound, no radio, open space waste disposal, and no television.
The top predictors of partial blindness among the aforementioned several variables are shown in Table 2. These factors include a mud floor, a wood-and-mud wall, cow manure, the absence of a radio, an unprotected well, a river or pond, irregular schooling, a lack of a telephone, and garbage dumped inside the property. With a p-value less than 0.05 and higher F-values of 38.649, these factors were highly significant (Annex 4).
The remaining factors, such as thatch roofs, absence of school attendance, lack of restrooms, open-air waste disposal, lack of a TV, burning inside the compound, public dump, river dump, and burning inside the compound, do not statistically contribute to partial blindness because their corresponding pvalues are higher than 5%.
|
Model variables (variables in percent) |
Unstandardized coefficients | Standardized coefficients | T | Sig. | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| (Constant) | 0.27 | 4.41 | 0.06 | 0.95 | |
| Mud floor | 0.16 | 0.05 | 0.21 | 2.93 | 0.003*** |
| Thatch roof | -0.01 | 0.02 | -0.03 | -0.66 | 0.51 |
| Wood/mud wall | -0.11 | 0.03 | -0.12 | -3.63 | 0.000*** |
| Cow dung | 0.07 | 0.01 | 0.21 | 5.96 | 0.000*** |
| Not attended schooling | 0.03 | 0.03 | 0.05 | 1.018 | 0.314 |
| Has no radio | 0.001 | 0.001 | 0.26 | 2.59 | 0.01*** |
| Unprotected well | -0.09 | 0.03 | -0.16 | -3.68 | 0.001*** |
| River/pond | -0.09 | 0.02 | -0.18 | -4.01 | 0.001*** |
| No toilet facility | -0.02 | 0.02 | -0.04 | -0.77 | 0.44 |
| Open space disposal | 0.04 | 0.063 | 0.077 | 0.56 | 0.57 |
| Non-regular schooling | 2.88 | 0.227 | 0.431 | 12.69 | 0.001*** |
| Has no telephone | -0.001 | 0.001 | -0.94 | -1.94 | 0.052 |
| Has no TV | 0.001 | 0.001 | 0.65 | 1.32 | 0.187 |
| Dumped inside compound | 0.002 | 0.001 | 0.21 | 3.11 | 0.002*** |
| Burned inside compound | 0.001 | 0.001 | 0.02 | 0.28 | 0.78 |
| Public dump | 0.03 | 0.06 | 0.03 | 0.41 | 0.68 |
| Dump to river | -0.19 | 0.11 | -0.08 | -1.75 | 0.08 |
| Burned inside compound | 0.03 | 0.07 | 0.04 | 0.43 | 0.67 |
| *** significant at P<0.05 | |||||
| Health Facility | Design | Distance (km) to the health facility | |||||||
|---|---|---|---|---|---|---|---|---|---|
| <1 | 1-4 | 5-9 | 10-14 | >=20 | Not stated | Total no of people | |||
| Hospital | N | 34,609 | 3,128 | 25,276 | 17,186 | 68,199 | 3,206,963 | 124,007 | 3,479,368 |
| % | 0.99 | 0.09 | 0.73 | 0.49 | 1.96 | 92.17 | 3.56 | 100.00 | |
| Clinic | N | 198,027 | 565,317 | 777,848 | 624,437 | 552,672 | 578,677 | 182,391 | 3,479,369 |
| % | 5.69 | 16.25 | 22.36 | 17.95 | 15.88 | 16.63 | 5.24 | 100.00 | |
| Health center | N | 205,818 | 556,289 | 841,642 | 509,985 | 591,320 | 590,863 | 183,452 | 3,479,369 |
| % | 5.92 | 15.99 | 24.19 | 14.66 | 17.00 | 16.98 | 5.27 | 100.00 | |
| Health post | N | 571,263 | 1,555,461 | 803,238 | 194,809 | 149,125 | 39,687 | 165,784 | 3,479,367 |
| % | 16.42 | 44.71 | 23.09 | 5.60 | 4.29 | 1.14 | 4.76 | 100.00 | |
| Pre /postnatal care | N | 1,009,717 | 2,680,195 | 2,448,004 | 1,346,417 | 1,361,316 | 4,416,190 | 655,634 | 13,917,473 |
| % | 7.26 | 19.26 | 17.59 | 9.67 | 9.78 | 31.73 | 4.71 | 100.00 | |
| Total | % | 7.256 | 19.26 | 17.592 | 9.674 | 9.782 | 31.73 | 4.708 | 100.00 |
| Source: Welfare Monitoring Survey Report (CSA, 2011) | |||||||||

| Outcome variable | Kolmogorov-Smirnova | Shapiro-Wilk | ||||
|---|---|---|---|---|---|---|
| Statistic | Df | Sig. | Statistic | Df | Sig. | |
| Blindness | .069 | 139 | .099 | .959 | 139 | .000 |
| Partial blindness | .046 | 139 | .200* | .985 | 139 | .119 |
| *. This is a lower bound of the true significance; a Lilliefors Significance correction | ||||||
| Model | Sum of Squares | Df | Mean Square | F | Sig. | ||
|---|---|---|---|---|---|---|---|
| 1 | Regression | 5722.421 | 15 | 381.495 | 13.745 | .000b | |
| Residual | 20149.992 | 726 | 27.755 | ||||
| Total | 25872.413 | 741 | |||||
| Model | R | R Square | Adj. R Square |
Std. Error of the Estimate |
Change Statistics | ||||
|---|---|---|---|---|---|---|---|---|---|
| R Square Change | F Change | df1 | df2 | Sig. Change | |||||
| 1 | .627a | 0.393 | .313 | 4.76 | .393 | 4.939 | 16 | 122 | 0.000 |
a. Predictors: (Constant), burned in side compound, non-regular schooling, thatch roof, has no TV, dumped inside compound, wood/mud wall, cow dung, public dump unprotected well, dump to river, no toilet facility, mud floor burned inside compound, , open space waste disposal; b. Dependent Variable: blindness.
| Model | Sum of Squares | Df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|---|
| 1 | Regression | 33942.537 | 18 | 1885.696 | 38.649 | .000b |
| Residual | 35275.171 | 723 | 48.790 | |||
| Total | 69217.708 | 741 | ||||
| R | R-square | Adjusted R Square | Std. Error of the Estimate | Change statistics | ||||
|---|---|---|---|---|---|---|---|---|
| R Square Change | F Change | df1 | df2 | Sig. change | ||||
| 0.7 | 0.49 | 0.478 | 6.98 | 0.49 | 38.649 | 18 | 723 | 0.000 |
Similarly, after standardization, the beta coefficients of the regression variables were adjusted after standardization. For instance, “has no telephone” and “has no TV” had the biggest contributions to partial blindness, with -0.936 and 0.644 units, respectively (Table 2). This indicated that the sources of information (education in various forms) had a significant impact on these people’s state of health.
Due to the modest p-value being smaller than 0.05 (Annex 4), the multiple linear regression model for partial blindness is significant overall. The corrected R-square was 0.478 when taking into account the model summary (Annex 5), demonstrating the model’s ability for explanation. This indicates that the predictor factors accounted for around 47.8% of the partial blindness model.
Only around 7% of the region’s residents live within a 1 kilometer radius of a health facility (Table 3), while 32% live more than 20 kilometers away from any health facility, not even a health post (first aid service center).
Energy use (cooking fuel types used in the household): Most Ethiopians use a mix of materials for cooking fuel. However, about 86.5% use firewood as a source of cooking fuel. The second and third most common fuels type used are dried dung and charcoal (37 and 18%, respectively).
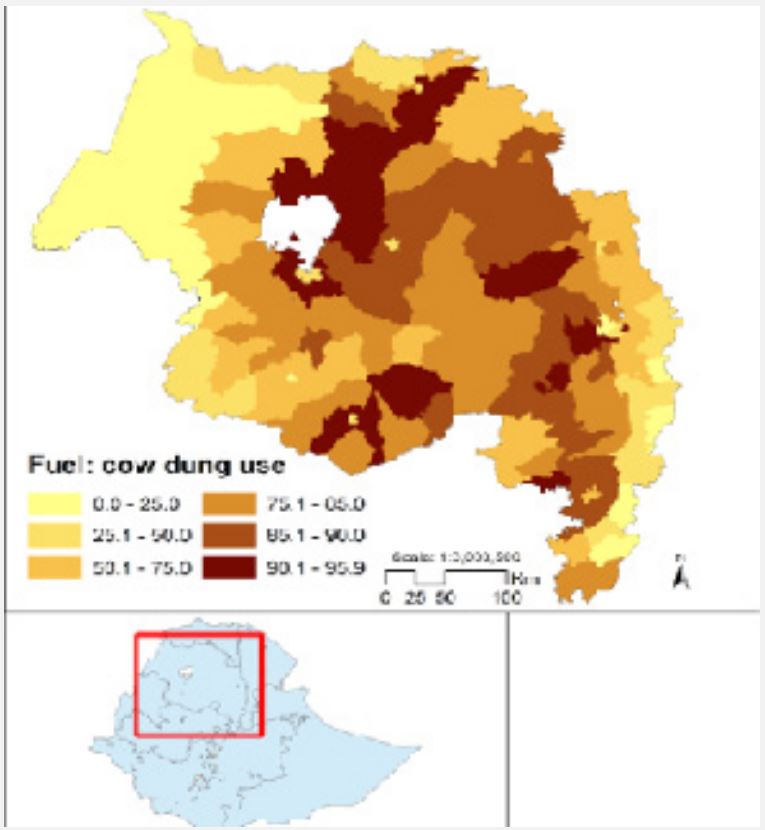
The use of firewood is ubiquitous, however, the majority of cow dung is only used as fuel in the highland regions of Amhara, Tigray, and Oromia (73, 47, and 30%, respectively - CSA-IFPRI, 2010). For about 16.6% of the overall population, other fuel sources like gas and biogas are the primary fuel source. In addition to being the primary source of energy in the rural area, cow dung continues to be a significant source of fuel for city dwellers in the highlands (Figure 3). Around 5,603,893 families in Ethiopia utilize cow dung as fuel, of which 2,810,424 (50.2%), both in rural and urban areas, were from the Amhara region (Figure 4).
Economic status: The majority of Ethiopians (92.1% of the country's population) reside in homes made with mud floors. More than 90% of the populace resides in homes with mud floors in every region, with the exception of Harari, Dire Dawa, and Addis Abeba. Thatch is primarily used to build roofs in Ethiopia, especially in the countryside. In comparison to 37% of the population who live in homes with corrugated iron roofs, more than 50% of the population lives in homes with thatch roofing (CSA-IFPRI, 2010). This suggests that the majority of rural residents have extremely low economic standing, making it difficult for them to maintain their health conditions, including their eye care, and to enhance their standard of living.
Education (information source): Radios are the most widely used medium of information in Ethiopia, where 38% of people live in homes with one. Only 4% of families had a phone, and only 6% of people lived in homes with a television (CSA, 2007). There were 14,476,781 persons without a phone, 14,241,209 without a TV, and 9,439,262 without a radio. And the Amhara region was home to roughly 26,126 persons, or nearly 29% of the population, who lacked such information sources. The majority of rural and elderly people find formal education to be a nightmare, which is unfortunate because it would greatly help to create a healthy society.
Infrastructure, environmental health and sanitation: In Ethiopia, access to healthcare facilities is generally limited in rural areas. Rural health care services in the Amhara region were widely spread and located distant from settlement areas. Access to health services is impacted by this. According to the CSA-IFPRI (2010), 10,061,697 dwelling units (households) lacked toilet facilities and relied on open space. 2,909,029 of them (or 29%) were discovered in the Amhara region. The Amhara region has 3,160,883 households (27%), out of the approximately 11,763,212 homes that use open space for trash disposal. That is, rural communities dump household garbage in nearby areas or on open land, which has an impact on both their human and environmental health.
Water sources and availability: Water access and sources have an effect on health consequences in general and eye diseases by limiting the cleanliness and sanitation of the communities. Rural communities lack sanitary amenities, health care facilities, and waste disposal systems and rely on open lakes or rivers for their daily water needs.
More than half of Ethiopia's population also gets the majority of its drinking water directly from bodies of water such lakes, ponds, and rivers (27%) or from unprotected wells and springs (28%). The majority of the drinking water in Somalia's and SNNP's southern regions comes from rivers and lakes. In all four major regions, unprotected wells are the main source of drinking water, however they are predominantly found in Somalia and Afar's more northern regions (CSA-IFPRI, 2010). In Tigray, Amhara, and southwest Oromia, protected wells and water taps (outside of dwelling blocks) were more common. Only 4% of the population in urban centers of the nation has access to the facilities; other drinking sources, such as water taps inside the house, are the main source of drinking water. Tap water is mainly available in metropolitan areas, especially in the Amhara region. However, in rural regions with limited access to water and sanitary facilities, sight problems are more common.
In the Amhara region, the use of cooking fuel like cow dung has a significant impact on blindness and partial blindness. Therefore, more research and assessment are needed to develop improvements to the situation as well as ways to replace cooking fuel and eliminate manure smoke, which was directly related to seeing difficulties, particularly in this area.
Blindness and partial blindness were both negatively impacted by the waste disposal systems (public dump, dumped inside the compound, and open access waste disposal), and the situation requires certain remedies. Naturally, this may be understood in the context of information access, which also contributed to blindness and partial blindness. The sanitary aspects (water source from unprotected wells, river/pond, absence of toilet facility, as well as access to health services) need to be deeply considered in order to ease the issues.
Lack of information access to media (lack of radio and telephone) has been barring the residents from having awareness of different means to protect preventable and curable diseases such as trachoma in the region according to the results of census reports under the disability category. Furthermore, the prevalence of partial blindness in the area was influenced by the construction of houses in the region using wood mud, a sign of a household's economic standing. That is, there may be a relationship between partial blindness and a household's economic situation that merits additional study
The other element is access to medical services, which also has a significant impact on vision problems (blindness and partial blindness), as these conditions are thought to be treatable if handled promptly. In comparison to other regions in the country with similar socioeconomic positions, statistics reveal that accessibility to the hospital (6%), accessibility to the clinic (68%), and accessibility to health centers (66%) is quite low. In other words, more than 90% of the population of the region cannot access hospitals, and one-third cannot access both clinics and health facilities. This suggests that accessibility to medical resources has evolved into a factor that influences both partial blindness and partial blindness.
Ethics approval and consent to participate: This is a secondary data analysis using census and sample datasets and didn’t require ethical approval and consent to participants.
Consent for publication: We used the sources of secondary datasets and acknowledge the providers of data used in these analyses.
Availability of data and materials: The datasets used and/ or analyzed during the current study are available from the corresponding author on reasonable request
Competing interests: We declare that there is no conflict of interest.
Authors’ contributions: The idea was conceived and initial data was organized by HS. Additional datasets and statistical analyses were done by LN. The draft was prepared by LN. The final report was written by both HS and LN. Both authors read, revised, and approved the ms.
Acknowledgment: We acknowledge organizations like the Central Statistical Agency, and national and regional offices for providing relevant datasets from different sources, and anonymous reviewers of this manuscript
