1PIDE School of Economics, Institute of Development Economics (PIDE), Islamabad, Pakistan.
2Department of Pharmacy, Quaid-I-Azam University, Islamabad, Pakistan.
Sameen Abbas
Email: sameenabbas21@yahoo.com
Received : Dec 24, 2022 Accepted : Jan 12, 2023 Published : Jan 20, 2023 Archived : www.meddiscoveries.org
A referral can be defined as a process in which a doctor or hospital does not possess sufficient resources (drugs, equipment, skills) to manage a clinical condition and it seeks for the assistance of a better or differently resourced facility at the same or higher level to assist the patient or take over the management of, the client’s case, which is not possible for the first hospital or doctor. All the Rural residence deserve access to health care services regardless of their place of residence with no exception. Nevertheless, rural communities are still experiencing a multitude of health problems in comparison with their urban counterparts. The objective of this study to identify challenges influencing implementation of referral system for quality health care service delivery and investigate the role of effective referral system in Rajan-Pur. The quantitative approach was used to explore the role of referral system is the district. Questionnaire was developed and used for data collection. After the assessment it was found that there is no implementation of proper rules and regulations of referral policy in the health system in district Rajanpur. In health utilization, resources were not present & utilized properly. Everyone wishes to go at tertiary care hospital for either he is suffering from chronic illness like cancer, heart disorder, and any other one or for minor ailment like fever, flu, cough etc. because no specialized care centers are available.
Keywords: Patient referral; Quality of care; Feedback; Health status; Pakistan; Primary health care; Rural health; Rural population; Dissatisfaction.
A referral system is a written request for specific medical services from the patient’s primary care physician to specialists regarding their illness. In order to receive any medical care, many Health Maintenance Organizations (HMOs) require a written referral from the patient. When a doctor or hospital encounters a problem with the provision of patient healthcare needs, the patient is referred to another facility for medical consultants [1]. This is because the doctor or hospital does not have enough resources (drugs, equipment, or skills) to manage a clinical condition and is looking for help from a facility that has better or different resources at the same or higher level to help the patient or take over the management of the client’s case, which is not possible for the first hospital or doctor. The referral system is helpful in health care provision and reduction health cost but one of the most important structural challenges of the health care system [2]. Referral methods play a major role in providing appropriate care for patients in many health care systems. The quality and efficiency in referral systems in Lower and Middle Income Countries (LMIC) are often undermined due to systemrelated inefficiencies such as poor infrastructure, relevant materials/equipment and insufficient skilled human resource [3].
Limited studies have evaluated barriers of the referral system for health care provision in rural areas [4]. Rural health provision has been a major concern of health ministry and government of Pakistan in recent years. Around half of the world’s seven billion inhabitants reside in rural areas. The population growth in rural areas necessarily requires the provision of extensive medical services and the consideration of physicians, nurse practitioners, midwifery, and other healthcare practitioners. There should be no exceptions for anyone living in rural areas who wants healthcare services available to them. However, compared to their urban counterparts, people in rural areas continue to face a wide range of health issues. Primary health care (PHC) is frequently used as the central approach to meet the medical requirements of rural areas around the world. Even though the idea of primary care has continued to remain viable as a means of providing access to medical facilities for everyone [5].
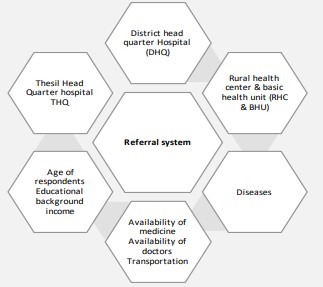
One of every person’s basic right is the ability to live in the best possible health. The majority of health systems around the world are hierarchical, starting with primary healthcare facilities, moving on to secondary healthcare settings, and ending with the highest level of health care facilities, which comprised of tertiary level facilities that offer specialized services [6]. However, the health referral systems across the various levels of care are generally quite underdeveloped in developing countries, which has an impact on the performance of the health system as a whole and contributes to unfavorable health outcomes. Based on the theory of change this conceptual framework has been constructed. Variables required for this purpose is referral system, income, age, transportation, availability of doctors and availability of medicine, educational background, relevant hospitals, and disease as shown in figure 1. Data related to these variables enable the researcher to access the performance of referral system for better health care provision or health service delivery [5,7].
A referral system is a fundamental requirement in health care. To increase access and raise the standard of services in a low-income nation, primary healthcare must be strengthened [8, 9]. However, it has been difficult to put into practice effective interventions to strengthen primary care, and many attempts have had limited success due to a lack of financial resources, a lack of political engagement, or insufficient maintenance of the referral patterns of patients using primary health centers and secondary hospitals [10]. So, this study aims to identify challenges influencing implementation of referral system for quality health care service delivery and investigate the role of effective referral system in Rajanpur.
The target population were patient’s approaching for treatment of three specific disease including tuberculosis, hepatitis, and cardio-related in the hospitals of Rajanpur district. The following hospitals from Rajanpur were included in this study,
• DHQ Rajanpur
• THQ Rojhan
• THQ Jampur
The following formula was used for sample size calculation [11].
Where:
n = sample size
z =standard normal deviation at required confidence level of 95%
E =desired margin of error
σ= expected standard deviation
So, by deriving a sample size, total of 249 patients as respondents were selected from 3 hospitals of Rajanpur district as mentioned above. Secondly, data was also collected from doctors of the same hospitals. 11 doctors were selected from three hospitals. Structured questionnaire was used to collect the data.
In patient related questionnaire, respondents were patient referred from different health care facilities. This part included demographic & socio-economic variables such as household status, educational level, and area of a patient. General health condition of a patient, from where patient get their first treatment, from where patient was referred was also noted. Overall cost of treatment including direct and indirect treatment such as registration fee, transportation cost, medicine cost and miscellaneous cost was the part of questionnaire. Through this questionnaire covered distance by patient to the referred hospital was evaluated. Doctors present in DHQ and THQ hospital were asked series of question including doctor personal information (name, designation, specialization). It also includes percentage of patient that visit via referral system and a number of patients he was checking each day in a hospital. This questionnaire of doctors also covered inflow of referred patients, catchment areas, and number of patients referred to specialized hospitals. Doctors and Referral Patients in district Rajanpur the Simple Random sampling technique was used Sample Size 273 sample size. States of questionnaire 249 patients from THQ and DHQ Hospitals, 11 doctors from THQ and DHQ Hospitals, and 13 doctors from BHU, MCH, and RHC’s. For the data analysis, frequency tables were made with SPSS version 26. used Crosstabulation and bar graphs to examine the variables' relationships. A pre-structured questionnaire is modified and adopted. The questionnaire was designed to take into account how culture works in the research area and to make sure it was written in a way that was clear and easy to understand. For data analysis, Excel and SPSS version 26 are used. Excel is used for data entry and generating graphs. Frequency tables are generated through SPSS.
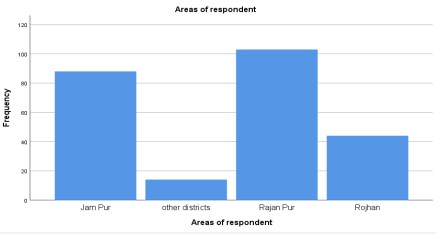
It was evaluated from Figure 2 that 103 patients which is 41.4% of total sample size belonged to Rajanpur zone visiting DHQ Hospital Rajanpur. 44 patients were from Rojhan and 88 patients from Jampur visiting tehsil headquarter hospital. Minimum number of respondents which is 5.6% of total sample size was from other nearby districts. It has been noted that most of the respondents came from flung areas where there was limited facility of transportation which was same assessed by Tanzil and her colleagues that these areas need their specialized centers and referral system do not work there [12].
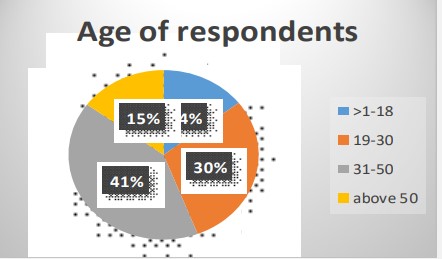
The age distribution of survey respondents is shown in the figure below (Figure 3). Age of respondents are taken four different categories less than 18 years old, 19 to 30, 31 to 50 years old and in last 50 and above.
The education level of a household member analyzes the level of awareness. Educational status of respondents was categorized as illiterate, primary, middle, matriculation, intermediate, bachelor and masters as mentioned in Figure 4.
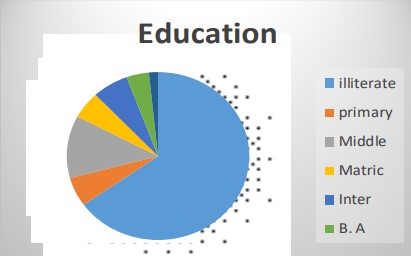
The educational statistics show that 65.1% respondents were illiterate. 5.6% respondents were with primary education level and 12.0% respondents had middle level education. 4.0% were at bachelors level. Only 1.6% out of total sample size had achieved master education.
It was noted that Cardiology patients in two THQ hospitals and in one DHQ hospital were 12% directly visiting hospital without any referral for treatment of cardiac problem. There were 45.4% of total number of Hepatitis B patients visiting hospitals. In addition, 2.4% patients were having Hepatitis B & C, 1.6% of Hepatitis B & D, Hepatitis C patients accounts for 14.9%, while only 1.2% were Hepatitis D patients. The number of Tuberculosis patients were 22.5% which is alarming.
| Disease | Valid percent |
|---|---|
| Cardiology | 12.0 |
| Hepatitis B | 45.4 |
| Hepatitis, B, C | 2.4 |
| Hepatitis, B, D | 1.6 |
| Hepatitis, C | 14.9 |
| Hepatitis, D | 1.2 |
| Tuberculosis | 22.5 |
| Total | 100.0 |
Specializations were observed like cardiologist, chest specialist, medical officer (MO) and senior medical officer (SMO) from under observed hospitals.
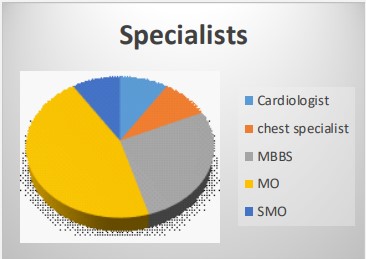
This shows that cardiologist and chest specialist were only 9.1% in observed hospitals, MBBS doctors were 27.3%, maximum number of doctors were medical officers (45.5%) while senior medical officers were 8% in this study. A contextual investigation of Health administrations foundation in Pakistan, regardless of an intricate system of more than 5000 fundamental health units and country health focuses, bolstered by higherlevel offices, essential health care exercises have not realized anticipated upgrades in health status, particularly of rustic populace gatherings [4]. An inadequately working referral system might be incompletely to fault. System investigation of patient referral was directed in a region of Punjab territory (Attock) to distinguish real inadequacies, assuming any, in this area [13].
Table 2 shows that total 11 doctors were interviewed from three hospitals under study. 3 were from THQ Jampur and Rojhan each while 5 were from DHQ Rajanpur. The number of refered patients to each doctor is maximum 20 from BHU, MCH and RHC. The findings also showed that direct visiting patients in these three hospitals was 30 minimum and 200 patients in one day. The average patients visit is 104.09% in a day. A cross sectional study conducted in Saudi Arabia attempted to recognize the gaps in the exploration on the effectiveness of referral forms for patients with sort 2 diabetes in Saudi Arabia and showed that there was no proper allocation of doctors to pursue with the referred as well as direct visiting patient [14] as our study.
| Major indicators | No. of doctors | Mean | Std. dev |
|---|---|---|---|
| Referred patients | 11 | 7.27 | 7.01 |
| Direct patients visit | 11 | 104.9 | 52.9 |
| Hepatitis, B, C | 2.4 |
This was also assessed that 9.1% respondents were refered from Maternal Child Health (MCH) center, 36.4% respondents out of total sample size refered from basic health units (BHUs), while most of the respondents i.e. 46% visited from THQ Jampur. RHCs rural health centers referred only 9.1% patients.
It was evaluated from interview with doctors that what percentage of patients they think could be treated at BHU level. The cardiologist response was 0% because of no facility of cardiac department at BHU, medical officer response was 9.1% due to presence of primary level facility, MBBS doctor response was 18.2%. Senior medical officer response was 90% that patients could be treated at BHU and no need of referal is needed. Using data from this study, we discovered that rural communities' needs are not being met by the current referral system. Furthermore, there were only a few specialists available in rural health centres, and they were not always available. The majority of the time, overcrowding makes patients wait a long time or visit a specialist's private office. The referral system is created to maximise the use of the three levels of healthcare services and to prevent wasteful use of resources at the specialised levels, including people and materials, and unnecessary congestion [5,12]. The referral system, however, has been ineffective due to specialty level restrictions and overabundance of non-urgent referred cases.
| Indicators | Mean | Std. Dev |
|---|---|---|
| Average no patients visiting you in a day? | 156.92 | 85.478 |
| what % of patients you attend & feel they need to be treated at your facility level? | 67.46 | 18.809 |
| How many patients need specialized testing investigations e.g., X.RAY/ECG | 2.92 | 1.441 |
| What % of patients do you feel should be referred to tertiary care hospitals? | 31.38 | 18.994 |
Health care facilities are limited in terms of resources availability and utilization whereas population is increasing rapidly over the time. The population growth is much faster than the growth rate of increasing facilities in Pakistan. In hospitals bed facility is not increasing parallel to population need. The way of implementation of referral system influences quality of health care process in rural areas. Although the referral system is thought to be completely effective, it constantly faces a number of difficulties. Everyone wishes to go at tertiary care hospital for either he is suffering from chronic illness like cancer, heart disorder, and any other one or for minor ailment like fever, flu, cough etc. The key issues of referral system in Rajanpur were lack of communication across hospitals and health care unities, reducing the effectiveness of referral system. Distance between hospitals is also a significant cause, where the patients were referred, which affect the effectiveness of referral system. The management of referral system on district level is almost silent and non-applicable due to lack of awareness.
Conflict of interest: The Author(s) declares(s) that there is no conflict of interest’.
