Obstetrician-Gynecologist and Maternal-Fetal Medicine Specialist, New York, USA.
Boris M Petrikovsky
Email: bpetriko@gmail.com
Received : Feb 20, 2026 Accepted : Mar 16, 2026 Published : Mar 23, 2026 Archived : www.meddiscoveries.org
Half a century ago, the womb was a “black box” - a space of mystery where fetal intervention was largely reactive and often too late. In the field of gynecology, many procedures remained invasive, with recovery times measured in weeks and outcomes clouded by a lack of gender-specific data. It was within this landscape that our research team began its journey.
Today, as we look back on 50 years of research and achievement, our research team was at the forefront of the technological shift that allowed us to see - for the first time the intricate development of the fetus. This mastery of imaging was not an end in itself, but a gateway. It led to the birth of fetal medicine as a surgical discipline, where our researchers pioneered techniques to treat life-threatening conditions in utero. By transforming the fetus into a patient in its own right, we moved from paradigm of “wait and see” to one of “diagnose and cure.”
Parallel to these breakthroughs in the womb, our work in gynecology has been a relentless pursuit of precision and preservation. We recognized early on that a woman’s health is not a subset of general medicine, but a distinct physiological ecosystem. Our team led the charge in developing minimally invasive surgical techniques that are now global standards, prioritizing individual management of symptomatic menopause and endometrial cancer screening. Below, please find the list of inventions and innovations developed by our research team under Professor Petrikovsky’s supervision and direct involvement.
Pet smear: George Papanicolaou landmark publication, “The diagnostic value of vaginal smears in carcinoma of the uterus” was published in 1941 in the American Journal of Obstetrics and Gynecology. Pap smear today is a standard of care for screening for cervical cancer.
Null Hypothesis: The goal of this pilot study is to assess the possibility of using menstrual flow smears to diagnose endometrial pathology. The purpose of this study is to develop a screening test for endometrial precancer and cancer.
Methods: 700 menstrual pads were studied for the presence of identifiable endometrial cells. Initial assessment was performed using a thin smear technique. Finally, a cell retrieval and suspension technique were used.
Results: Normal menstrual patterns were identified in 688 cases, suspicion of hyperplasia in 21, and suspicion of cancer in one case. Endometrial hyperplasia was confirmed in 7 patients; endometrial cancer was detected in 1.
Conclusions: Menstrual smears do have a diagnostic potential in screening for endometrial cancer. In simple words, we asked patients to deliver their used menstrual pads for histological diagnosis. We called it Pet smear after the principal investigator Dr. Petrikovsky. Research data was first published in 2000.
Recently, American Cancer Society recommended self collected vaginal smears as a primary screening method for cervical cancer. These tests are being performed privately at home. If high risk HPV is detected, a clinician-collected follow up sample is needed. Pet smear, however, is totally different because the target of screening is endometrial cancer and collection material - used pads containing cells in menstrual blood.
Soft Forceps: The risk of maternal and fetal trauma and, fear of lawsuits, have contributed to a significant decline in forceps deliveries and an increase in rates of cesarean sections. For example, around 60-65% of all births in Brazil are by cesarean section, far above the WHO recommendation (around 10%).
Robson Classification: Even in low-risk groups (Robson groups 1 & 2) which are favorable for vaginal birth, cesarean section rates are high (3 times higher than international norms).
Healthcare system factors: In private settings, obstetricians are often paid per procedure, incentivizing quicker cesarean sections over vaginal deliveries, which are more time consuming.
“Soft” forceps were designed by Dr. Petrikovsky in collaboration with doctors from NYU School of Medicine and Russian Federation State University. The idea is simple - to cover metal blades with soft rubber in order to protect birth canal and fetal head from metal blades of forceps.
To create the soft forceps the blade portion of the forceps was dipped 2 or 3 times for 5 min in a multipurpose rubber coating resin (Performix: Circle pines, Minn) to provide a soft coating. This rubber cover added 1.5 mm to the thickness of the blades (patent pending). The institutional review board approved the use of the soft forceps and informed consent was obtained in each case. Following the American College of Obstetrician and Gynecologist guidelines, a low forceps delivery with a Simpson model were performed in all cases.
Study concluded that “soft” forceps significantly reduced the rates of neonatal facial abrasion, skin bruises, as well as damage to the birth canal.
In utero partial heart transplantation-application for research grant: This work is done with collaboration with L. Neymotin, PhD and A. Ureash MD, PhD (Mount Sinai Medical Center, Miami, FL).
Rationale: Fetuses with congenital heart anomaly (e.g., hypoplastic left heart) die soon after birth. Potential heart donors are anencephalic fetuses.
Although no human in utero heart transplantation has yet been performed, the surgical, physiologic, and immunologic foundations required for such a procedure are now sufficiently developed to make it technically plausible. Placental circulation provides continuous cardiopulmonary support, and the fetal immune environment offers a unique opportunity for tolerance induction. Advances in fetal surgery and microvascular techniques further support the feasibility of cardiac replacement during gestation.
The arguments for in utero partial heart transplantation are derived from multiple independent scientific observations:
• Immunologic permissiveness of fetal development,
• Stabilizing effects of placental physiology,
• Redefined capabilities of contemporary fetal surgery,
• Positive practical results of partial cardiac transplantation in newborns,
• Precedent of successful in utero kidney transplantation, demonstrating that solid-organ fetal transplantation is possible.
Citi screen-individualized computer-assisted cancer screening: The most successful cancer screening programs are based on the identification of precursor lesions (e.g., cervical intraepithelial neoplasia, with cervical cancer and polyps for colorectal malignancy. This is based on the Vogelstein theory of carcinogenesis, based on the model of linear progression from precancer to a localized early-stage cancer, which allows ample time for early detection and management.
In designing successful screening program, we rely on modified Wilson and Jungner principles. CitiScreen is using American Cancer Society guidelines but goes beyond it. CitiScreen algorithm is protected by copyright and designed for individual cancer screening based on the patient’s history, tumor markers and genetic screening.
Screening for cancer is the most deficient area of the healthcare system. Many cancers are slow growing, which allows ample time for early detection. In cancer statistics, the earlier the stage at detection, the better the outcome. Thus, a five-year survival of stage one ovarian cancer is over 95% while for stage four, it is less than 5%.
US Preventive Task Force currently recommends screening for a limited number of cancers (colon, cervix, breast, and prostate). For smokers at age 50 plus, lung cancer screening should be discussed with the doctor. According to US Preventive Task Force recommendations, most screening programs end around the age of 70-75 despite the fact that age is the most significant risk factor for screening.
How CitiScreen Works?
The goal of CitiScreen is to put together fragmented screening protocols by creating computer algorithms for the following cancers: lung, ovarian, breast, prostate, cervix, thyroid, colorectal, pancreas, and skin, among others.
CitiScreen steps of cancer screening:
• Screening for risk factors (family history, medical history, lifestyle, smoking, tanning, etc.)
• Genetic Screening (testing for genetic predisposition)
• Screening for cancer precursors (cervical dysplasia for cervical cancer, complex endometrial hyperplasia for endometrial cancer, etc.)
• Blood screening for early-stage cancers (tumor markers)
• Diagnostic smears if indicated (Pap, urinary, mouth, etc.)
Screening results are used for individual screening algorithms which comes with practical recommendations, eq. frequency of colonoscopy, need for MRI screening, etc. CitiScreen algorithms are constantly updated based on changes, circumstances (age, new cases in the family, changes in living habits, etc.) and new advancements in the science of cancer screening. CitiScreen subscribers receive yearly screening recommendations on the frequency and type of screening modalities.
In utero neurological examination of the fetus: The ability of the newborn to ambulate is related to the level of the defect in the spinal canal, eq spinal bifida. Typically, levels caudal to L2 are necessary for ambulation with long braces. Fetal ultrasound is able to determine the site of the spinal defect but does not predict future function.
The technique of simulating leg withdrawal has prognostic power in predicting later ambulation. It may not be universally helpful until about 20 weeks gestation. The test was developed in collaboration with Dr. S Pavlakis, a pediatric neurologist at Maimonides Medical Center.
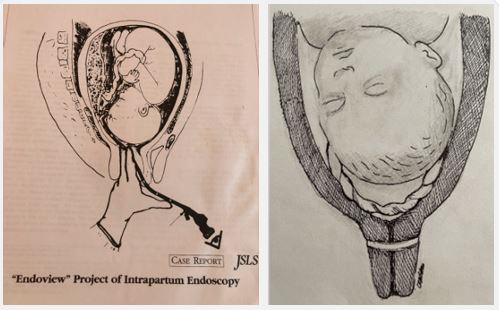
Intrapartum hysteroscopy: The idea of inserting an endoscope into the uterine cavity in late pregnancy and labor was developed and patented in 1981. The endoscope was inserted into the uterus via the cervix after spontaneous or artificial rupture of membranes.
The main stages of the endoscopic examination are the following: for observation of the presenting part, the fibroscope is inserted to 15-25 cm; for observation of the fetal neck, for possible looping of the umbilical cord, the fibroscope is inserted to 20-25 cm; for observation of the fetal torso and extremities, and for placental visualization, the fibroscope is inserted to 40 45 cm. The procedure lasts for not more than 15 minutes and is well tolerated by the patient.
Intrapartum endoscopy to be worth performing in selected cases for the following purposes: 1) To determine precisely the nature and type of umbilical cord loops. 2) To predict with accuracy of the size of the fetus (based on correlation between the size of small parts and fetal weight). 3) To investigate the possibility of undetected meconium in the hindwaters. 4) To evaluate the integrity of the uterine scar in patients undergoing a trial of labor after prior cesarian section. Successful attempts have been made to remove meconium from the fetal pharynx.
Prevention of the umbilical cord prolapse in fetuses with funic presentation: A funic presentation is defined as the presence of the umbilical cord below the presenting part and can be detected by both transabdominal and transvaginal sonography. A funic presentation is a risk factor for umbilical cord prolapse. The prolapse of the umbilical cord complicates 1 in 400 pregnancies and has been associated with high perinatal mortality. We propose a new approach-the placement of a third-trimester cervical cerclage in women with persistent funic presentation. The cervical cerclage mechanically closes the cervix, which prevents the presenting umbilical cord to prolapse.
Use of patient’s ovarian tissue collected during operative procedures in reproductive age to treat symptomatic menopause when patients got older: Menopause is a manifestation of reproductive aging. Today, most women live beyond 80 years and spend 30-40% of their lives being postmenopausal. In the 1980s and 90s, Hormonal Replacement Therapy (HRT) was administered to millions of women to relieve menopausal symptoms. However, some women have contraindications to take it. HRT is also associated with increased risk of breast and endometrial cancer.
In this study, we compared the age of onset of menopause between women who had Ovarian Tissue (OT) harvesting as part of gynecologic or obstetrical procedure with women who had similar procedures without OT harvesting. In no instance was a surgical procedure performed for the sole purpose of OT harvesting. Ovarian harvesting was performed by removing about 20% of one ovarian cortex. The ovarian cortex was cryopreserved via a slow freezing protocol. Then, at the request of the patient, after having symptomatic menopause, all cryopreserved tissue was transplanted. Every OT transplantation was performed subcutaneously, in the axilla, under local anesthesia. Subsequently, women who underwent OT transplantation were questioned to whether they received a relief from menopausal symptoms (hot flashes, heart palpitations, vaginal dryness, sleep issues, mental issues).
Rremoval of about 20% of ovarian cortex for the purpose of delaying menopause in healthy women does not seem to be associated with POI and heterotopic ovarian tissue transplantation seems to successfully reverse menopausal symptoms. The removal of about one fifth of the ovary does not appear to damage the ovarian reserve to induce a significant loss of year of ovarian function. As ovarian reserve decreases with age, the freezing of a portion of the ovarian cortex guarantees a duration of endocrine function restoration directly dependent on the age in which the OT is removed. For the harvesting of OT to postpone the menopause to be feasible, the reduction of ovarian functioning determined by ovarian biopsy must be less than the years of longevity given by the tissue transplantation.
Development of in-utero fetal pacemaker: A notable cause of hydrops is a complete atrioventricular conduction block that may be the result of autoimmune diseases such as systemic lupus erythematosus and Sjogren’s syndromes. Neonatal lupus erythematosus is an isoimmune disease that occurs with passage of anti-Ro/SS-A and anti-La/SS-B antibodies through the placenta. These antibodies travel through the fetal circulation binding to fetal tissue causing congenital heart blocks and non cardiac neonatal lupus. Lab studies in NLE show elevated liver enzymes and thrombocytopenia.
In collaboration with Dr. M Ovadia from pediatric cardiology we developed an animal model of utero pacemaker. It is known that hydrops with a third-degree heart block approaches a mortality of 100% despite treatment with steroids. The prospect of fetal pacing should be further explored as a treatment option for congenital complete heart block. Interventional pacing and heart rate support should correct the hemodynamic derangement. This fetal pacing system should avoid umbilical cord complications by bypassing umbilical vasculature and prevention of cord knotting.
In our study, complete AV block was induced with ethanol in 11 Sprague rats. A J-wire was advanced through a 1cm subcostal incision and across diaphragm into the thorax. A pacing lead was then passed over the J-wire and positioned in close proximity to the mediastinum. Pacing was successful in 10 of the 11 rats with ventricular capture and QRS widening. The mean QRS complex changed from 50.2 ms pre-pacing to 95.1 ms post-pacing. There were no complications caused by deployment. Movement of the fetus was also considered as a mode of deployment failure, but it is well known that a hydroptic fetus ceases to move thereby reducing the risk of dislodgement.
Therefore, intrauterine pacing should provide the greatest efficacy in reducing fetal demise. The monolithic fetal pacemaker holds the greatest potential for success. Recent studies in this field have recognized the importance of fetal pacemakers as an early intervention of hydrops. Further exploration of fetal heart pacing is imperative in regards to the future of interventional fetal medicine.
First ever in utero platelets transfusion to the fetus with risk of hemorrhage: Congenital thrombocytopenia is a part of a number of fetal disorders and puts fetus at risk of hemorrhage and death. In 1993 we encountered a fetus with TAR syndrome, a rare inherited disorder characterized by hematological thrombocytopenia (with absence of hypoplasia of megakaryocytes, a leucoerythroblastic blood smear, and anemia) and limb (absence of radii) abnormalities.
In collaboration with doctors from the pediatric hematology division, we performed in utero transfusion of irradiated (3000 rads), apheresis platelets. Upon delivery of the neonate, characteristic TAR syndrome orthopedic anomalies of the upper extremities with normal hands and digits were confirmed. The platelet count on cord blood was 152,000 per mm, testifying to the success of the procedure.
This was the first reported case of prenatal infusion of platelets to treat the fetus with TAR syndrome and prevent perinatal hemorrhage.
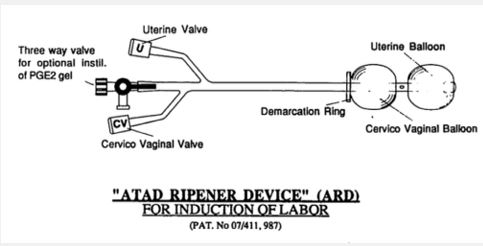
Ripening of the unfavorable cervix and induction of labor with balloon device: Today using the balloon for cervical ripening and induction of labor is an everyday procedure, and very few know that Dr. Petrikovsky, in collaboration with physicians from Carmel Hospital (Haifa, Israel) pioneered this technique.
The double balloon device is held in place and the dilator vector is applied by the two balloons inflated on both sides of the cervix, one toward the other. In our report, no cases of accidental rupture of membranes, chorioamnionitis, or placental abruption were caused by use of a catheter. The procedure was convenient and well tolerated by most women.
The findings of the present study indicate that ripening of the cervix might have been caused by the device itself. The locations of the two inflated balloons in both sides of the cervix might have caused mechanical pressure on the cervix, with the pressure vectors in the direction of the cervix, thus dilating and effacing it. Indeed, dilation and effacement were the Bishop score parameters affected most by the ripener device.