1Pingyi County People’s Hospital, Linyi City, Shandong Province 273300, China.
2The First college of Cinical Medical Sciences, China Three Gorges University, YiChang 443000, China.
3Hospital of Traditional Chinese Medicine of Three Gorges University, Yichang 443003, China.
Shengmei Wu
Email: 411564292@qq.com
Received : Feb 17, 2026 Accepted : Mar 11, 2026 Published : MMar 18, 2026 Archived : www.meddiscoveries.org
Background: Chronic wounds, including venous ulcers and diabetic foot ulcers, impose significant clinical and economic burdens globally. Compression therapy is a cornerstone intervention, yet its optimal application timing and management strategies lack standardized guidelines.
Methods: According to the ‘6S’ evidence resource model, evidence retrieval is searched from the top-down and collected relevant guidelines, best practices, evidence summaries, systematic reviews and expert consensus. The retrieval time limit was from the database establishment to 20 March 2025. Two reviewers independently screened and evaluated the literature, and then extracted and summarized the evidence according to the JBI grading of evidence and recommendation system.
Results: This study summarizes 18 pieces of evidence in 7 aspects, including indications, contraindications, application, assessment, management strategies, effectiveness, and adverse reactions, related to the application timing and management strategies of compression therapy for chronic wounds.
Conclusions: Compression therapy significantly enhances chronic wound healing but requires rigorous contraindication screening and dynamic pressure adjustment. Clinicians should adopt evidence-based protocols integrating ABI assessments and patient education. Future innovations should focus on smart devices and longitudinal outcome tracking.
Keywords: Chronic wound management; Compression therapy; Venous ulcers; Evidence based guidelines; Contraindications.
Chronic wounds are clinically defined as “injuries that fail to achieve anatomical integrity and functional restoration after 4 weeks of standardized wound management” [1], his category encompasses pressure injuries, diabetic foot ulcers, venous ulcers, and arterial ulcers. Epidemiological data reveal a global prevalence of 1.5%2% for chronic wounds [2], with diabetic foot ulcers accounting for 1.03% prevalence and approximately 9.1 million new cases annually [3], Notably, venous ulcers affect 4% of the population aged over 65, demonstrating a rising incidence trend due to population aging and increasing metabolic disease burden. Recent statistics indicate that global healthcare expenditure on chronic wound management has reached US$89 billion annually, constituting 3.18% of total medical costs [4,5]. Beyond economic burdens, patients frequently endure recurrent pain, infection risks, psychological distress, and potential limb amputation, significantly compromising quality of life [6,7]. With advancements in precision medicine and nursing science. Compression Therapy has emerged as a cornerstone intervention for chronic wounds (e.g., venous leg ulcers, lymphedema). Its mechanism involves dual path regulation through hemodynamic optimization and molecular modulation: Graduated pressure delivery (4050 mmHg at ankle decreasing to 15-20 mmHg proximally) enhances venous pump function, reduces venous hypertension (40% decrease in capillary leakage), while suppressing inflammatory cytokines and promoting fibroblast proliferation with collagen remodeling [8-10]. Both the International Union of Phlebology (UIP) and European Wound Management Association (EWMA) recognize compression therapy as the gold standard for venous ulcer management [11]. Nevertheless, clinical implementation faces challenges including undefined therapeutic windows, inadequate contraindication screening protocols, and lack of personalized pressure adjustment guidelines, resulting in variable compliance and therapeutic outcomes. The absence of robust evidence-based protocols and standardized operational frameworks substantially hinders clinical application. This study aims to systematically review and synthesize existing evidence on compression therapy for chronic wounds, thereby establishing a scientific foundation for standardized clinical practice.
Establishment of the problem: The PIPOST tool, developed by the Evidence-Based Nursing Center at Fudan University, was utilized to establish a problem related to evidence-based practice. The patient Population (P) targeted for the application of evidence consisted of individuals suffering from chronic wounds. The Intervention (I) implemented was compression therapy. Clinical medical personnel served as the Professionals (P) utilizing the evidence. The Outcomes (O) monitored after implementing the evidence encompassed factors such as the duration of wound healing, recurrence intervals, frequency of recurrence, and overall quality of life. Evidence was applied in various Settings (S), including hospitals, community environments, and home settings. The types of evidence (T) considered comprised guidelines, best practice methodologies, expert consensus, evidence summaries, systematic reviews, and original research studies.
Literature retrieval strategy: According to the ‘6S’ evidence resource model, evidence retrieval is searched from the top-down. The databases searched included: BMJ Best Practice, Up to Date, National Institute of Health and Clinical Excellence (NICE), National Guideline Clearinghouse, Guideline International Network, Scottish Intercollegiate Guidelines Network, Registered Nurses’ Association of Ontario, Chinese Med live Guideline Network (CMGN), Australian JBI Evidence Based Health Care Database, Cochrane Library, PubMed, CINAHL, Embase, Web of Science, China Biology Medicine, China Knowledge Resource Integrated Database (CNKI), Wan fang and VIP. Relevant professional websites include the Wound, Ostomy and Continence Nurses Society, WOCN website, World Council of Intrastromal Therapists, WCET website, European Venous Forum, EVF website, European Society for Vascular Surgery, ESVS website, Association for the Advancement of Wound Care, AAWC website, Health Service Executive, HSE website. The search terms were created based on the combination of Medical Subject Headings and free terms, and the literature search formula consists of three parts: the first of which was frailty or other manifestations of frailty, the second was intervention/management/prevention or specific measures and the third was a restriction on the type of literature to be searched, as shown below:( compression therapy OR pressure therapy OR elastic bandages OR compression stocking* ) AND (chronic wound* or nonhealing wound* or hard healing wound* or pressure ulcer* or bedsore* or pressure sore* or pressure injury* or decubitus ulcer* or varicose ulcer* or venous ulcer* or stasis ulcer* or diabetic foot or diabetic feet or arterial ulcer* or scar* or scar formationor lymphedema) AND (guideline* OR ‘practice guideline’ OR routine* OR ‘recommended practice’ OR ‘evidence summary’ OR consensus* OR ‘systematic review’ OR ‘meta-analysis’). The search timeframe is from database inception to 20 March 2023.
Literature inclusion and exclusion criteria: The inclusion criteria were as follows: (i) Adult patients (≥18 years old) with a clear diagnosis of chronic wounds (including venous ulcers, diabetic foot ulcers, arterial ulcers or pressure injuries) and receiving compression therapy intervention, regardless of gender, race or underlying diseases; (ii) literature types included guideline, best practice, evidence summary, systematic review and expert consensus; (iii) language was either Chinese or English. The criteria for exclusion from the study encompassed two primary conditions. (i) any literature categorized as a conference abstract, guideline interpretation, research plan or proposal, or outdated guides that have since been superseded was not included. This ensures that only relevant and contemporary sources are considered to maintain the integrity of the research; (ii) materials that contained incomplete information, whose full texts could not be accessed, or that exhibited a low quality of evaluation were also excluded from the analysis. These criteria were established to enhance the reliability and validity of the findings by focusing solely on high-quality and complete scholarly works.
Study selection and data extraction: Two reviewers conducted a thorough and independent screening of the literature collected, adhering strictly to predetermined inclusion and exclusion criteria. In situations where disagreements arose between the reviewers regarding the selection of studies, discussions were held to reach a consensus. If a consensus could not be achieved through discussion, a third author was consulted to provide an impartial resolution. Following this screening process, the same reviewers proceeded to extract data independently, utilizing a standardized data extraction form to ensure consistency and reliability in their approach. Importantly, during this phase, each reviewer was blinded to the other’s data extraction process to minimize bias. The extracted data encompassed essential characteristics of the studies, including information such as the first author’s name, their affiliated institution, the year of publication, the source, the type of evidence presented, and the specific topic addressed in the article.
Literature quality evaluation criteria
Guideline: The Appraisal of Guidelines for Research and Evaluation (AGREE II) tool was utilized to assess the quality of the guidelines that were included in this study [12]. This evaluation framework comprises a total of 23 distinct items categorized across six different domains. Each item is rated on a Likert scale ranging from 1 to 7, where a score of 1 indicates strong disagreement with the statement and a score of 7 signifies strong agreement. To provide a comprehensive assessment, the score for each domain is expressed as a standardized percentage, which is calculated based on the cumulative scores assigned to each individual item within that domain. The formula for determining the standardized percentage for each field is as follows: it involves taking the obtained score for the domain, subtracting the least possible score, and then dividing that result by the difference between the maximum and least possible scores, finally multiplying by 100 to obtain a percentage representation [13].
Systematic reviews: The systematic reviews that were incorporated into the analysis underwent a thorough evaluation utilizing the AMSTAR 2 tool. This tool comprises 11 distinct entries designed to assess various aspects of systematic reviews
Each of these entries was categorized based on specific criteria, resulting in ratings of ‘yes’, ‘no’, ‘unclear’, or ‘not adopted’. This rigorous assessment process provides a comprehensive overview of the methodological quality and reliability of the systematic reviews included in the study. In addition to the evaluation of systematic reviews, a consensus among experts was sought to further enhance the understanding and credibility of the findings. This consensus is critical, as it offers a collective agreement among professionals in the field, ensuring that the conclusions drawn from the systematic reviews are not only robust but also aligned with current best practices and expert opinions in the relevant domains.
Expert consensus: The assessment of the quality of the expert consensus included in this study was conducted utilizing the Expert.
Consensus Standard, which was established in 2016 by the Joanna Briggs Institute (JBI) Centre for EvidenceBased Health Care located in Australia. This evaluation tool encompasses six specific items that allow for a nuanced judgment, providing responses categorized as ‘yes,’ ‘no,’ ‘unclear,’ or ‘not applicable.’ These categories enable a structured approach to evaluating the consensus quality, ensuring a comprehensive analysis of the expert opinions considered in the study.
Best practice and evidence summary: In conducting a quality evaluation of best practices and evidence summaries, we revisited the original literature that forms the foundation of the evidence presented. This thorough examination allowed us to identify and select appropriate evaluation tools that were aligned with the specific types of literature we encountered. By ensuring that the evaluation instruments correspond to the literature type, we enhance the reliability and relevance of our assessments, ultimately leading to a more robust understanding of the practices in question.
Literature quality evaluation process: The quality evaluation process was carried out by two independent reviewers, both of whom possess expertise in evidence-based nursing. Their systematic examination of the relevant literature allowed them to assess the quality and relevance of the studies in question. In situations where the reviewers reached differing conclusions, a third individual, experienced in evidence-based research, intervened to make the final decision. This additional layer of review ensured that the evaluation process remained rigorous and grounded in sound methodology. Furthermore, when disagreements arose regarding the conclusions drawn from the extracted evidence, the reviewers adhered to a specific set of principles for inclusion. These guidelines prioritized the utilization of evidence that was firmly established within an evidence-based framework. Additionally, they emphasized the importance of selecting high-quality studies to ensure the reliability of the findings. Finally, they focused on incorporating the most recently published and authoritative literature, thereby ensuring that the evaluation was not only based on solid ground but also reflective of the latest advancements and insights in the field. This comprehensive approach to quality evaluation reinforces the integrity and credibility of the findings presented.
Criteria for determining evidence level & recommendation level: The evidence included in this study was rigorously evaluated and categorized using the JBI grading of evidence and recommendation system. This system assigns evidence grades based on the type of research design, resulting in a classification that ranges from levels 1 to 5. Additionally, the evaluation is guided by the FAME framework established by JBI, which assesses the feasibility, appropriateness, meaningfulness, and effectiveness of the evidence presented. Through this comprehensive evaluation process, the level of recommendation for each piece of evidence is determined, distinguishing between A-level recommendations, which are considered strong endorsements, and B-level recommendations, which are viewed as weaker endorsements.
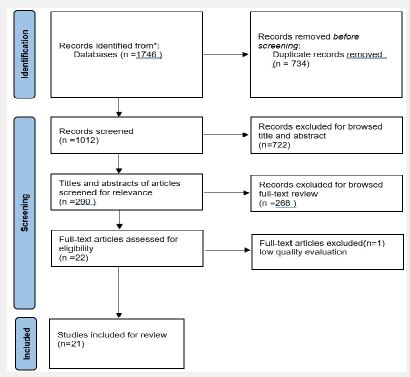
General characteristics of the included literature: The initial search resulted in 1,746 articles. After excluding duplicates and those that did not meet the requirements after reading the title, abstract and full text, a total of 21 publications were finally included, including 4 guidelines [14-17], 1 best practices [18], 4 expert consensuses [19-22], 3 evidence summaries [23-25], and 9 systematic reviews [26-34].
The study selection process is presented in (Figure 1), and the general information of the included literature is shown in (Table 1).
| Included literature | Year | Type of evidence | Literature sources | Topic of the literature |
|---|---|---|---|---|
| Sun et al. | 2025 | Guideline | PubMed | Clinical guidelines on compression therapy in venous diseases |
| Ratliff et al. | 2022 | Guideline | WOCN | Compression for lower extremity venous disease and lymphedema |
| Ito et al. | 2025 | Guideline | Web of science | Guidelines for the management of lower leg ulcers and varicose veins, second edition |
| Valesky et al. | 2024 | Guideline | Web of science | Diagnosis and treatment of venous leg ulcers: S2k Guideline of the German Society of Phlebology and Lymphology (DGPL) |
| Shi et al. | 2021 | Systematic Reviews | Cochrane Library | Compression bandages or stockings versus no compression for treating venous leg ulcers |
| de Moraes Silva et al. | 2024 | Systematic Reviews | Cochrane Library | Compression for preventing recurrence of venous ulcers |
| Mirakhmedova et al. | 2023 | Systematic Reviews | Embase | Daily duration of compression treatment in chronic venous disease patients: A systematic review |
| Ferguson et al. | 2024 | Systematic Reviews | PubMed | Decision-making on the use of compression hosiery and compression bandaging: a systematic review |
| Li et al. | 2022 | Systematic Reviews | PubMed | Breast Cancer: A Meta-analysis of Randomized Controlled Trials |
| Declan Patton et al. | 2023 | Systematic Reviews | Web of science | A meta-review of the impact of compression therapy on venous leg ulcer healing |
| Nischwitz et al. | 2020 | Systematic Reviews | Embase | Evidence-based therapy in hyp-ertrophic scars |
| Walsh et al. | 2023 | Systematic Reviews | Embase | Keloid treatments: An evidence-based systematic review of recent advances |
| García-Chico et al. | 2025 | Systematic Reviews | Web of science | Wrapping up the evidence: Bandaging in breast cancer-related lymphedema |
| Vignes et al. | 2021 | consensus study | Web of science | Primary lymphedema French National Diagnosis and Care Protocol |
| E. Rabe et al. | 2020 | consensus study | PubMed | Risks and contraindications of medical compression treatment |
| Finlayson et al. | 2023 | consensus study | Embase | Priority topics for chronic wound research in Australia: A consensus study |
| Lurie et al. | 2022 | consensus study | PubMed | The American Venous Forum, American Vein and Lymphatic Society and the Society for Vascular Medicine expert opinion consensus on lymphedema diagnosis and treatment |
| Li et al. | 2022 | Best evidence summary | VIP | Best evidence summary for intermittent pneumatic compression in treatment of patientswith breast cancerrelated lymphedema |
| Mu et al. | 2022 | Best evidence summary | CNKI | Summary of the best evidence for self-management in patients with venous leg ulcer |
| Zheng et al. | 2020 | Best evidence summary | VIP | Evidence summary of compression therapy in patients with venous leg ulcer |
| Ruiz et al. | 2024 | a best practice | JBI | Compression therapy in patients with venous leg ulcers: a best practice implementation project |
Note: WOCN: Wound, Ostomy, and Continence Nurses Society; JBI:Joanna Briggs Institute
Quality evaluation results of the included literature
Quality evaluation results of the guidelines: There were 4 guidelines included in this study [14-17]. Four guidelines have ≥60% percentage of standardization
in six fields, with a recommendation level of A. The results of the standardized scores for each domain and the 177 overall quality evaluation of the guidelines are shown in (Table 2).
Quality evaluation results of systematic reviews
In all, 4 literatures were evaluated as high quality, five as medium quality. Detailed quality evaluation contents are shown in Table 3.
| Guidelines | Percentage of standardization in each area (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Scope purpose | Participant | The rigor of the designation | Clarity of expression | Applicability | Editorial independence | Quality score | Recommendation level | |
| Sun et al. | 95 | 70 | 85 | 90 | 75 | 80 | 82.5 | A |
| Ratliff et.al. | 94 | 89 | 85 | 92 | 78 | 83 | 86.8 | A |
| Takaaki-Ito et al. | 88 | 83 | 92 | 94 | 75 | 100 | 88.7 | A |
| Valesky et al. | 90 | 85 | 75 | 90 | 76 | 77 | 82.2 | A |
Note: Standardization percentage of each field = (obtained score - minimum possible score)/ (maximum possible score - minimum possible score) × 100%; Recommendation level: if the standardized percentage of six fields is >60%, it is 181 highly recommended (level A); if >3 areas have a standardised percentage > 30% and < 60% are recommended (level B); if 182 there are ≥3 areas with a standardised percentage < 30%, it is not recommended (level C).
| Methodological quality evaluation results of systematic review | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| systematic review | Evaluation entry | Overall quality | ||||||||||
| ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | ⑧ | ⑨ | ⑩ | ⑪ | ||
| Declan-Patton et al. | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | No | Yes | Medium |
| Shi et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | High |
| Moraes-Silva et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | High |
| Li et al. | Yes | Yes | Yes | No | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Medium |
| Sevara-Mirakhmedova et al. | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | No | Unclear | Yes | Medium |
| Ferguson et al. | Yes | Unclear | Yes | Unclear | Yes | Yes | Yes | Unclear | No | No | Yes | Medium |
| Nischwitz et al. | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | No | Unclear | Yes | High |
| Walsh et al. | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | No | No | Yes | Medium |
| García-Chico et al. | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Methodological quality evaluation of expert consensus | |||||||
|---|---|---|---|---|---|---|---|
| Expert consensus | Evaluation entry | Overall quality | |||||
| ① | ② | ③ | ④ | ⑤ | ⑥ | ||
| Kathleen Finlayson et al. | Yes | Yes | No | Yes | Yes | Yes | High |
| Rabe et al. | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Hettrick et al. | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Lurie et al. | Yes | Yes | No | Yes | Yes | Yes | High |
Four expert consensus articles were independently evaluated by two evaluators according to JBI expert opinion quality evaluation tool, and the overall quality of the articles was medium or high, so they were approved for 189 inclusions. Detailed quality evaluation contents are shown in Table 4.
Quality evaluation results of the best practice and evidence summary: For quality evaluation of 1 best practices and 3 evidence summaries.The one recommended practice is all from the JB I Evidence-Based Health Care Center, and the original evidence level and recommendation strength are directly selected,we reviewed and evaluated the original literature on which the evidence was based, and the overall quality was high, all included in this study.
Summary and description of evidence: The evidence was extracted from the final literature, and the evidence was evaluated by JBI grading of evidence and recommendation system. Through the induction and integration of the evidence, the evidence was finally summarised from seven aspects. There are a total of 31 pieces of evidence, including indications, contraindications, application timing, evaluation, management strategies, effectiveness and adverse reactions.
Note: ABI: Ankle-Brachial Index; CDT: Complete Decongestive Therapy; CEAP: Clinical-Etiology-Anatomy Pathophysiology; DVT: Deep Vein Thrombosis; EVTA: Endo venous Thermal Ablation; IPC: Intermittent Pneumatic Compression; ISL: International Society of Lymphology; MRI/ MRA: Magnetic Resonance Imaging/Magnetic Resonance. Angiography; NYHA: New York Heart Association; PAD: Peripheral Arterial Disease; POSAS: Patient and Observer Scar Assessment Scale; QoL: Quality of Life; VTE: Venous Thromboembolism.
Comprehensive assessment before applying compression therapy for chronic wounds is the cornerstone
Based on the evidence from items 1-3 in (Table 5) [14 25], this study systematically reviewed the indications and contraindications of compression therapy for chronic wounds. The evidence is derived from evidence summaries and expert consensus, with a relatively high level of evidence, which is of high value in guiding the clinical practice of compression therapy for chronic wounds. The evidence in this study shows that the research emphasizes that a multi-dimensional assessment must be completed before implementing compression therapy, including core elements such as medical history collection (underlying diseases, medication history), wound characteristics (type, stage, infection status), and hemodynamic indicators (ankle-brachial index, venous function testing). It is particularly important to note that for patients with combined arterial disease (ABI< 0.8), a modified compression protocol should be used to avoid the risk of tissue ischemia. In clinical practice, it is recommended to establish a standardized assessment process by integrating objective detection indicators (such as Doppler ultrasound) with subjective symptom assessment (pain VAS score) to achieve precise treatment decisions.
Items 4-8 in (Table 5) [14,15,17,19,25], summarize the application timing and assessment focus of compression therapy for chronic wounds. The evidence sources are relatively rich and have strong guiding significance for when to apply and how to assess before compression. For example, for venous ulcers, compression treatment should be initiated immediately after diagnosis, with daily compression time ≥ 6 hours, and maintained for life after healing. For active venous ulcers, compression should be started before getting up in the morning and continued until going to bed. When standard pressure therapy is ineffective, intermittent pneumatic compression pumps can be combined. Additionally, assessing the wound before applying compression therapy is fundamental, including clinical symptom assessment, objective examination assessment, and subjective assessment. In the management of chronic wounds, the application timing of compression therapy directly affects the healing process and the risk of complications.
Dynamic adjustment of management strategies requires balancing safety and efficacy, and formulating personalized management plans is key
Items 10-15 in (Table 5) [16,17,20,29,33], summarize the evidence related to the management strategies of compression therapy. The stratified management strategy based on evidence emphasizes pressure precision, technology combination, and material adaptation. For active venous ulcers, elastic bandages with a pressure of 40-50 mmHg are recommended, which promote lymphatic return by increasing the hydrostatic pressure in the tissue space. For mixed arterial and venous lesions (ABI>0.5), non-elastic materials (such as short-stretch bandages) can reduce the risk of ischemia by 50%, which is related to the more uniform pressure distribution of non elastic materials at rest. Studies have shown that Intermittent Pneumatic Compression (IPC) combined with elastic bandages can reduce lymphedema volume by enhancing interstitial fluid return and promoting lymphatic vessel contraction [25]. For patients with difficulty in putting on and taking off, adding a double-layer gradient stocking (18-24 mmHg) can increase comfort by 30% under equivalent pressure, but the long-term skin tolerance still requires follow-up data support [21]. After assessment of infectious ulcers, using silver ion dressings combined with compression can reduce the bacterial load of infectious ulcers by 99%, and low-allergenic materials (such as polyurethane) can reduce the incidence of contact dermatitis from 8-12% to less than 2%. Standardized compression therapy can increase the healing rate, shorten the healing time, reduce pain in DVT patients within 24 hours after compression, and improve the quality of life. In summary, compression therapy has certain efficacy in the treatment of chronic wounds, but clinical medical staff should closely monitor the patient’s response and potential risks when using it, and formulate personalized plans based on the patient’s condition. Future research can further explore the best application methods of compression therapy in the treatment of different types of chronic wounds and how to reduce adverse reactions and improve treatment effects.
Compression therapy can effectively promote the healing of chronic wounds. Ensuring patient safety is the key point
Evidence 17-18 in (Table 5) [15,17,18,20,21,24,27,29,33], summarizes the effectiveness and adverse reactions of compression therapy in treating chronic wounds. The research evidence shows that compression therapy can effectively promote the healing of chronic wounds, and the evidence comes from multiple systematic reviews, with good quality. However, current evidence also indicates that during the application of compression therapy, adverse reactions such as contact dermatitis, skin irritation, temporary skin numbness, and erythema may occur. Improper application may also lead to complications such as soft tissue damage, aggravated arterial ischemia, and nerve damage. Therefore, healthcare providers can adopt the following strategies to ensure the safety of compression therapy for chronic wounds: ① Strictly control the application scope of compression therapy; ② Control the compression pressure and duration; ③ Pay attention to observing the patient’s skin and blood circulation during the application process; ④ Closely monitor the patient’s vital signs and subjective feelings; ⑤ Develop emergency plans, including the handling procedures for equipment failure and sudden changes in the patient’s condition, to ensure the safety of compression therapy. Additionally, in the management of burn scars, a pressure of 30-40 mmHg may inhibit scar hyperplasia, but long-term follow-up data is lacking, and further exploration is needed in the future. Existing evidence shows that compression therapy can effectively increase the cure rate of chronic wounds and shorten the healing time of chronic wounds, with high quality evidence and good guiding significance. At the same time, compression therapy has good safety [15,29,34]. In conclusion, compression therapy has certain therapeutic effects in the treatment of chronic wounds, but healthcare providers should closely monitor the patient’s response and potential risks during use and develop personalized treatment plans based on the patient’s condition. Future research can further develop intelligent compression devices to improve patient compliance and explore how to reduce adverse reactions and improve treatment effects. Patient reported outcomes have certain significance in the field of healthcare. On the one hand, patient-reported outcomes emphasize patient-centered care, focusing on the patient’s feelings and needs, making medical decisions more in line with the patient’s expectations and needs, and helping to improve patient satisfaction and trust. On the other hand, patient-reported outcomes can provide the necessary information for formulating individualized chronic wound treatment plans. By understanding the patient’s symptoms, functional status, quality of life, and nutritional status, health problems can be identified in a timely manner, treatment plans can be adjusted, and treatment effects can be improved [35]. Therefore, future research should focus on the impact of compression therapy on patient reported outcomes in chronic wound patients.
This study summarizes 21 pieces of evidence in 7 aspects, including indications, contraindications, application, assessment, management strategies, effectiveness, and adverse reactions, related to the application timing and management strategies of compression therapy for chronic wounds. The results of this study indicate that compression therapy can be used as an adjunctive treatment for chronic wound management. Clinical practitioners should fully assess the application scope and timing of compression therapy and, based on the specific clinical context, consider the feasibility, appropriateness, clinical significance, and effectiveness of the evidence, and apply the evidence in combination with the patient’s preferences to promote the healing of chronic wounds. Further high-quality research is still needed in the future to improve the quality of evidence and focus on the effect of compression therapy on patient-reported outcomes in chronic wound patients.
Abbreviations
ABI: Ankle-Brachial Index; AAWC: Association for the Advancement of Wound Care; AGREE II: Appraisal of Guidelines for Research and Evaluation II; AMSTAR 2: A Measurement Tool to Assess systematic Reviews 2; BMJ: British Medical Journal; CDT: Complete Decongestive Therapy; CEAP: Clinical-Etiology Anatomy-Pathophysiology; CMGN: Chinese Med live Guideline Network; CNKI: China National Knowledge Infrastructure; CVI: Chronic Venous Insufficiency; DGPL: German Society of Phlebology and Lymphology; DKZF: German Cancer Research Center; DVT: Deep Vein Thrombosis; EDL: Essential Diagnostics List; EMBASE: Excerpta Medica Database; ESVS: European Society for Vascular Surgery; EVF: European Venous Forum; EVTA: Endo venous Thermal Ablation; EWMA: European Wound Management Association; FAME: Feasibility, Appropriateness, Meaningfulness, Effectiveness; HIS: Hospital Information System; HRV: Heart Rate Variability; HSE: Health Service Executive; IPC: Intermittent Pneumatic Compression; ISL: International Society of Lymphology; JBI: Joanna Briggs Institute; LLM: Large Language Model; MRA: Magnetic Resonance Angiography; MRI: Magnetic Resonance Imaging; NICE: National Institute for Health and Care Excellence; NIH: National Institutes of Health; NYHA: New York Heart Association; PAD: Peripheral Arterial Disease; PD: Parkinson’s Disease; PDI: Patient Dignity Inventory; PIPOST: Population Intervention Professionals Outcomes Settings Type of evidence; POSAS: Patient and Observer Scar Assessment Scale; QoL: Quality of Life; SW-CRT: Stepped Wedge Cluster Randomized Trial; UIP: International Union of Phlebology; VAS: Visual Analogue Scale; VIP: VIP Database; VTE: Venous Thromboembolism; WCET: World Council of Intrastromal Therapists; WOCN: Wound, Ostomy, and Continence Nurses Society.
Ethics approval and consent to participate: This analysis is based on publicly available published data, and no additional ethical approval is required as it does not involve any direct human or animal experimentation.
Consent for publication: Not applicable
Competing interests: The authors declare that they have no competing interests.
Funding: The authors did not receive support from any organization for the submitted work.
Authors’ contributions: Qianqian Peng contributed to the conceptualization, methodology, and drafting of the manuscript. Sheng Mei Wu, as the corresponding author, oversaw the literature review, data collection, analysis, and manuscript revision. Xian Wu assisted with literature review, data collection, and manuscript editing. Lili Zhang contributed to data curation and analysis. Yanli Hu participated in study supervision and methodological guidance. Bangyan Yao provided methodological support and manuscript revisions. Ying Lei contributed to manuscript editing and project administration. All authors reviewed and approved the final version of the manuscript.
Acknowledgements: Not applicable.
Key points
A total of 18 best-evidence recommendations on compression therapy for chronic wounds were systematically summarized from seven domains (indications, contraindications, timing, assessment, management strategies, efficacy, and adverse effects) based on the “6S” evidence resource model.
The evidence provides a standardized framework for initiating compression therapy, adjusting pressure parameters, and integrating adjunctive therapies.
