1Private practictioner, Vittorio Emanuele, 352 - 98037 Letojanni (ME), Italy.
2Shedir Pharma Group SpA, Via Bagnulo, 95 – 80063 Piano di Sorrento (NA), Italy.
3Neilos Srl, Via Bagnulo, 95 – 80063 Piano di Sorrento (NA), Italy.
Maria Potenza
Email: m.potenza@neilos2015.com
Received : Nov 21, 2025 Accepted : Dec 23, 2025 Published : Dec 30, 2025 Archived : www.meddiscoveries.org
Osteoarthritis (OA) is considered the most common musculoskeletal disease, affecting more than 240 million people worldwide. Most patients develop OA in the lower joints, such as knee or hip. Nearly 30% of individuals over the age of 45 show radiographic evidence of knee (Gonarthrosis) and hip (Coxarthrosis) OA. Ypsodol® is an innovative nutraceutical specifically formulated with a new patented technology called F.A.G.® (fatty acids group), representing a new approach to counteract the inflammation and pain as natural treatment alternative with pharmacological ones.
A total of 35 patients with gonarthrosis, coxarthrosis, cervicoarthrosis was enrolled in the present retrospective clinical survey and were orally treated with Ypsodol® monitoring the efficacy on pain perception and joint mobility using four different standard questionnaires. After only three months of treatment a good reduction in all parameters related to pain perception was obtained and after six months of treatment with Ypsodol® a further implementation of pain relief was registered. Also, for joint mobility after six months of treatment, Ypsodol® improved of about 76% the motion score without any significant side effect.
The present study suggests that Ypsodol® could be considered a promising nutraceutical approach in order to counteract pain and inflammation in osteoarticular disease after a more complete and extensive clinical validation.
Keywords: Osteoarticular disease; Pain; Nutraceuticals; Anti-inflammatory effect.
Osteoarthritis (OA) is considered the most common musculoskeletal disease, affecting more than 240 million people worldwide. Most patients develop OA in the lower joints, such as knee or hip. Nearly 30% of individuals over the age of 45 show radiographic evidence of knee (Gonarthrosis) and hip (Coxarthrosis) OA. The prevalence of both symptomatic and radiographic OA is higher in women (over 18%) than in men (under 14%), indicating that age and female gender are significant risk factors [1].
OA is a disease that leads to cartilage loss. It was traditionally thought to result solely from increased mechanical stress on a joint (e.g., overload on weight-bearing joints or anatomical joint incongruence) or from cartilage matrix fragility (e.g., due to genetic alterations). Chondrocytes (the only cells in cartilage) have very low metabolic activity and limited capacity to repair tissue. Unlike other tissues, articular cartilage cannot mount a typical inflammatory response when damaged because it is avascular and not innervated. However, the discovery that soluble mediators such as cytokines and prostaglandins can stimulate chondrocytes to produce Matrix Metalloproteinases (MMPs) marked the beginning of the “inflammatory” theory of OA. Experimental data have shown that subchondral bone also plays a crucial role in OA, both as a mechanical buffer and as a source of inflammatory mediators that contribute to pain and degradation of the deep cartilage layers [2].
Joint swelling, a clinical feature of OA, is often attributed to inflammation and reflects synovitis, which may result from synovial thickening or fluid accumulation. Multiple studies suggest that synovitis may indicate more severe disease and is associated with an increased risk of radiographic progression. Systemic levels of High-Sensitivity C-Reactive Protein (hs-CRP) reflect synovial inflammation in OA patients and are associated with pain levels [3].
The exact reason why the synovium becomes inflamed in OA remains debated. The most widely accepted hypothesis suggests that synovial cells react by producing inflammatory mediators found in the synovial fluid. These mediators can activate chondrocytes in the superficial cartilage layer, leading to MMP production and increased cartilage breakdown. They also induce synovial angiogenesis and stimulate further production of inflammatory cytokines and MMPs by synovial cells—thus creating a vicious cycle. In this way, synovitis perpetuates cartilage degradation in OA [4,5].
Cervicobrachialgia is often associated to OA and several studies evidence how this type of disease is common in worldwide population. It is a disease caused by compression of the nerve roots of the brachial plexus, often due to herniated cervical discs, osteoarthritis or other cervical pathologies. The lifetime prevalence of cervicobrachialgia pain is notably high (22-70%), with a marked increase in women entering their fifth decade of life [6].
Cervicobrachialgia includes different types of pain, with different origins: Nociceptive pain, Neuropathic pain and Nociplastic pain [7,8].
Many professional guidelines emphasize disease prevention to reduce reliance on medications. Preventive strategies include weight loss and avoiding excessive physical stress. If prevention is insufficient or if symptoms are severe, pharmacological treatment becomes necessary. The main drug options include: Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), COX-2 inhibitors, corticosteroid injections, Intra-articular Hyaluronic Acid (HA) injections or serotonin-norepinephrine reuptake inhibitors. All these pharmacological treatments often present typical side effects that reduce patients’ compliance and consequently the therapeutic effect [9].
Therefore, the scientific research is globally oriented to novel therapeutic approach in different fields with the aim to maximise the efficacy and patients’ compliance reducing side effects [10-17]. Ypsodol® is an innovative nutraceutical specifically formulated with a new patented technology called F.A.G.® (fatty acids group), representing a new approach to counteract the inflammation.
F.A.G.®, has been found to be involved in cell protection from oxidative stress and inflammation. In cultured human monocytes, F.A.G.®, is non-toxic up to 1 mg/mL and has been shown to inhibit the release of inflammatory cytokines induced by a lipopolysaccharide challenge [18,19]. The acronym F.A.G.®, includes a number of different mixtures obtained by a calibrated mixing of long and short chain fatty acids given to sustain the metabolism of macrophages involved in the inflammatory reaction with the aim of facilitating its resolution and the shift of macrophages to the non-pro-inflammatory phase. Different mixtures have been studied and proposed in relation to different pathologies in different body districts and the specific inflammatory reaction elicited in the pathology.
The aim of the present study was to evaluate the efficacy and safety of Ypsodol® administration in patients with different chronic osteoarticular diseases after three and six months of administration monitoring different parameters related to pain and joint motion ability.
An Italian medical doctor with a specialization in orthopedy, enrolled participants in the period October 2024-May 2025 evaluating their clinical manifestations during medical examination.
In particular, the participants were selected according to defined inclusion criteria related to the presence of an osteoarticular disorder: gonarthrosis, coxarthrosis, cervicoarthrosis.
Considering these clinical conditions, a total of 35 patients were enrolled in the present survey; at the first medical examination, the doctor reported for each patient its age, gender, weight, comorbidity and use of pharmacological treatments. Regarding pharmacological treatments, the main class used were antihypertensives. The use of oral analgesics or NSAIDs concomitantly to Ypsodol® administration was not reported.
At the enrolling time (T0) patients were evaluated according to different standardized questionnaires: Ritchie Index, Present pain Index, pain intensity scale, limitation movement scale.
Then, each participant administered Ypsodol® according to the posology reported in the product leaflet with the evaluation of the sub mentioned questionnaires at the follow-up visits after three months (T3) and six months (T6).
Settings
The clinical survey has been conducted by an Italian medical doctor and is based on its clinical experience in patients taking Ypsodol®. The retrospective observational survey was conducted in accordance with the Standards of Good Clinical Practice of the European Union and the ethical principles expressed in the Declaration of Helsinki. Data were retrospectively collected in in the period October 2024-May 2025 by the medical specialist. Ethical approval was not necessary according to National Code on Clinical Trials declaration because this data derives from a real-life retrospective study [20].
The aim of the present study was to evaluate the effect of Ypsodol® oral administration after three months (T3) and six months (T6) of treatment.
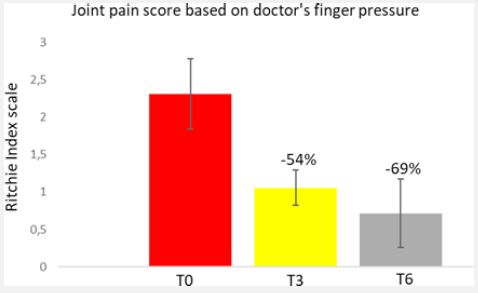
Different standardized questionnaires can be clinically used in case of OA, such as Ritchie Index that is useful to make an assessment of the tenderness of 26 joint regions that is based on the summation of joint responses after applying a digital pressure. Conventionally the range used for individual measures is 0-3 where 0 represents patient reported no tenderness, 1 patient complained of pain, 2 patients complained of pain and winced, 3 patients complained of pain, winced and withdrew [21].
As reported in figure 1, the mean value for Ritchie Index at T0 was very high (about 2.3 score), while after the administration of Ypsodol® after only three months of treatment this value was reduced of about 54%. Continuing the therapy with the nutraceutical product the value was still reduced of 69% obtaining results with a medium score of 0.71, indicating according to Ritchie Index a minimum pain perception.
Also considering the Present Pain Intensity index (PPI), results after Ypsodol® administration were very interesting. PPI is a simple, 1-5 scale used to measure pain intensity as part of the McGill Pain Questionnaire (MPQ) were 1 corresponds to no pain and 5 to excruciating pain [22].
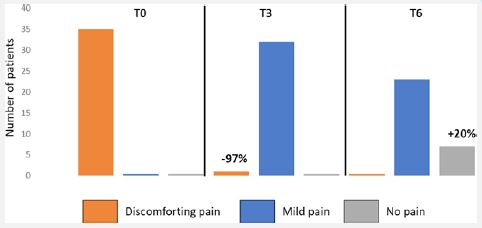
In fact, as reported in figure 2, at the enrollment time quite all patients showed discomforting pain while this number was sensibly reduced already at T3 with a big part of the patients that changed their pain score to mild pain (about 91% of the total population enrolled in the study). After six months of treatment with Ypsodol®, about 20% of the population showed a no pain score and no patients had a discomforting pain.
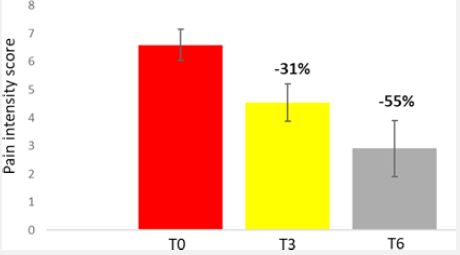
The Pain intensity scales comprise a group of different scale for pain based on a unidimensional measure of pain intensity that are widely used in adult population including for osteoarticular disorders with higher scores indicating higher pain intensity [23].
Also, according to pain intensity scale a reduction of about 55% after six months of administration of Ypsodol® was reached; and it’s important to underline that at T3 the pain perception of the patients was already reduced of about 31% with respect to T0 indicating also a rapid analgesic effect (Figure 3).
Finally, another test related to articular motion was applied in order to understand if the joint mobility was also influenced by Ypsodol® administration.
For the applied test, a score of 0 corresponds to no motion while higher scores correspond to better motion with 10 score representing the maximum joint activity.
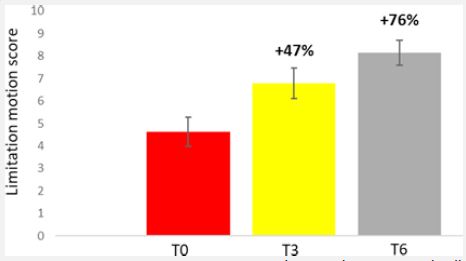
As deducible from figure 4, an increase of 47% and 76% of the joint motion with respect to the enrolment time (T0) was achieved at T3 and T6 respectively demonstrating a complete anti- inflammatory and analgesic effect of Ypsodol® after its administration in patients starting from very low values of joint mobility.
The present data are consistent with scientific literature regarding the oral administration of fatty acids for pain relief effect [24].
Moreover, the specific and patented fatty acids group formulation in Ypsodol® seems to have a very rapid effect already after only three months of treatment that was further implemented continuing the treatment for six months on pain perception as well as on joint mobility. The present study presents some limitations that must be implemented with following studies comprising a broader patient’s population and the evaluation of plasmatic parameters related to inflammation markers for example C reactive protein, and or Erythrocyte sedimentation rate.
A total of 35 patients with diagnosed of osteoarticular diseases like gonarthrosis, coxarthrosis, cervicoarthrosis was enrolled in the present retrospective clinical survey and were orally treated with Ypsodol® monitoring the efficacy on pain perception and joint mobility using four different standard questionnaires. After only three months of treatment a good reduction in all parameters related to pain perception was obtained and after six months of treatment with Ypsodol® a further implementation of pain relief was registered. Also, for joint mobility after six months of treatment, Ypsodol® improved of about 76% the motion score without any significant side effect.
The high therapeutic efficacy of Ypsodol® is due to the patented technology F.A.G.® able to achieve a strong anti-inflammatory effect modulating the mast cells and macrophage activity giving a rapid and enduring pain relief effect implementing joint mobility too.
The present study suggests that Ypsodol® could be considered a promising nutraceutical approach in order to counteract pain and inflammation in osteoarticular disease after a more complete and extensive clinical validation.
Conflicts of interest: We declare that Umberto Di Maio is a Shedir Pharma Group S.p.A. member and Maria Potenza is a Neilos S.rl. member.
Funding: This research was funded by a grant from Neilos S.r.l.
Authors’ contributions: All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
