1Department of Medicine, Faculty of Medicine, Tbilisi State Medical University, Georgia.
2Senior Consultant-High Risk Obstetrician and Laparoscopic Surgeon, Georgia.
Sakina Sakina
Tel: +995-595773293;
Email: sakmub828@gmail.com
Received : Sep 23, 2025 Accepted : Oct 20, 2025 Published : Oct 27, 2025 Archived : www.meddiscoveries.org
Background: Mullerian duct anomalies are categorized as a cluster of congenital structural malformations in the development of Müllerian ducts, thus rendering infertility in women. Unicornuate uterus also known as a banana-shaped uterus, is a type of mullerian anomaly wherein only a single mullerian duct develops in place of the physiologically arising two-sided pear-shaped uterus. Furthermore, a non-communicating rudimentary horn uterus presents as a rare mullerian variation, herein developmental complications display a uterine mimicking structure with abnormal endometrial tissue growth. Research shows that genetic and environmental factors are attributed to the cause of these reproductive organ disruptions. Overall, affected females incur significant risks of infertility, miscarriages, endometriosis, menstrual issues, preterm birth and urogenital deformities.
Case presentation: We present a rare case of successful unicornuate uterus pregnancy: 28-year-old female patient with chronic infertility, preliminary diagnosed non-communicating rudimentary horn uterus conception by the route of transperitoneal passage of sperm and simple serous cystadenoma.
Conclusion: Circumventing the odds, this obstetric case evinces prompt medical assistance, intraoperative and postoperative medical interventions in aiding a successful preterm childbirth to a patient with rare Müllerian duct anomalies.
Keywords: Mullerian duct anomalies; Unicornuate uterus and Infertility.
A giant ovarian cyst is defined as a cyst which is greater than 10 cm in diameter from radiological examination or if the size of the cyst tends to exceed the umbilicus. Extra-large benign cysts and malignant cysts of the ovary are found to be rare [1]. Unicornuate uterus is a rare mullerian abnormality, and it is potentially associated with a rudimentary horn [2]. An unicornuate uterus with a rudimentary horn is a rare type of congenital uterine anomaly that occurs when one of the Müllerian ducts fails to develop properly. This condition affects about 0.4% of women. The rudimentary horn can be either communicating, where it connects to the main uterine cavity, or non-communicating, where there is no connection between the two [2]. Pregnancy in a rudimentary horn is an extreme and rare type of ectopic pregnancy as it is associated with a risk of spontaneous rupture and bleeding due to increased uterine blood flow [2]. We report the successful diagnosis and management of a unique case of unicornuate left uterus pregnancy of a patient found to have a large ovarian cyst and a right non-communicating rudimentary horn abnormality who presented with prolonged infertility.
A 28-year-old female patient, was referred to the hospital with a history of chronic infertility and formerly diagnosed 10 cm left ovarian cyst through Ultrasonography (USG). However, it’s noteworthy to mention that no remarks on her uterine morphology were recorded in the USG reports. Adhering to the above findings, the patient was advised to undergo a laparoscopic ovarian cystectomy.
The key in situ findings of the laparoscopic surgery performed under general anesthesia are as follows-
1. Left ovary with two cysts of 5 × 5 cm dimensions.
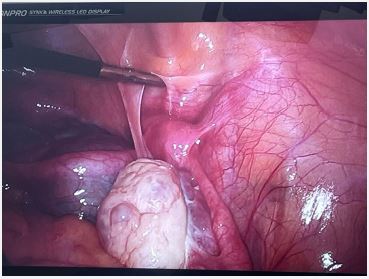
2. Left Unicornuate uterus (Figure 1).
3. Chromotubation dye test proved right non-communicating rudimentary horn uterus with a high-lying right ovary (Figure 2).
In the view of (I/v/o) absent availability of an informed consent for the excision of right non-communicating rudimentary horn uterus, only a left ovarian cystectomy was successfully performed with histo-pathological reports suggestive of (s/o) simple serous cystadenoma.
Post surgery patient (pt.) was advised to conceive naturally and was prescribed Dehydroepiandrosterone (DHEA) a hormone supplement to potentially improve her diminished ovarian reserves, as clinical biochemistry tests for Anti-Mullerian Hormone (AMH) revealed AMH values of 1.20 ng/ml indicating low fertility.
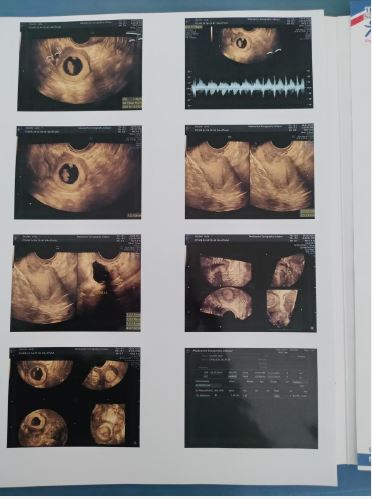
Succeeding three months of amenorrhea, Pt. came to the hospital with a positive home urine pregnancy test (home UPT). USG performed at 7 weeks of gestation revealed a rare inception of pregnancy in the right non-communicating rudimentary horn uterus. The aforementioned finding was remarked by the light of transperitoneal passage of sperm (Figure 3).
Laparoscopic excision of the right rudimentary horn was accorded i/v/o the risk factors associated with a pregnancy established in non-communicating rudimentary horn uterus. The key In situ findings of laparoscopic surgery performed under general anesthesia was s/o unremarkable right and left ovaries in succession to a left unicornuate uterus adequate to establish a healthy pregnancy.
After 4 months the patient conceived naturally in the left unicornuate uterus. Due to the prominence of preterm labor in unicornuate uterus pregnancies, cervical cerclage was performed at 14 weeks of gestation. Following appropriate antenatal care, the patient underwent emergency Lower Segment Caesarean Section (LSCS) i/v/o breech presentation of the fetus. She delivered a male child with an APGAR score of 8/10 at first minute and 9/10 at fifth minute.

Ovarian cysts are a frequent gynecological problem that affects at least 1 in 5 women, according to research. Though they can form at any stage of life, they are most frequently observed during the reproductive years, especially around menarche. The body’s normal hormonal fluctuations are frequently the cause of this [4]. Most cysts during this time are called functional cysts, as they are linked to the regular menstrual cycle, and they often tend to resolve without the need for medical treatment [4]. Ovarian cysts are not only found in younger women but are also found in women with post menopause. In fact, studies have shown that about 21.2% of healthy women in Europe have them [4].
The majority of the symptoms that ovarian cysts might produce tend to worsen gradually as the cyst grows. One of the most particular symptoms is the progressive enlargement of the abdomen, which is frequently felt as bloating or fullness. Many women experience a dull, persistent, and often unpleasant pain in the lower abdomen, even though it’s not usually severe or localized [4]. In women experiencing post menopause or women who are not able to menstruate, unexpected vaginal bleeding is expected in such cases [4]. As the cyst begins to develop, it tends to add pressure on the surrounding organs. Constipation, nausea, vomiting, consistent urge to urinate, and an early feeling of being full after eating a small quantity can all result due to this pressure [4].
Diagnosis may be delayed because these symptoms can occasionally be mistaken for those of other illnesses. While they are extremely uncommon overall, ovarian tumors are the most prevalent kind of cancer affecting the teen reproductive system [4].Every year, an estimated 2.6 out of 100,000 women are diagnosed with an ovarian tumor [4]. In girls under the age of seventeen, 10–30% of ovarian tumors are malignant. About 1% of all children cancers and 8% of pediatric abdominal tumors are caused by them [4].
The ability to diagnose these cysts has greatly improved due to advancements in imaging, particularly transvaginal ultrasonography.
Doppler studies help to assess blood flow, which is important for ruling out cancer [3]. CT and MRI scans tend to be used for more complicated cases. Blood tests like CA-125 can be done to confirm a diagnosis even if they are usually not specific [3].
The course of treatment is completely dependent on the size and type of the cyst. While functional cysts may not require treatment at all, large or more symptomatic cysts might require surgery [3]. Laparoscopic cysts removal is done more prominently as it promotes faster recovery. In some scenarios, hormonal therapy might help to prevent recurrence [3].
Our case involved a large left ovarian cyst that was discovered by MRI. On laparoscopy, two cysts measuring about 5 × 5 cm each were found in the left ovary, along with a left unicornuate uterus and a non-communicating right rudimentary horn with a high-lying right ovary. A dye test confirmed free spill on the left side only, and a left ovarian cystectomy was performed. Histopathology revealed a simple serous cystadenoma.
A unicornuate uterus is a rare congenital uterine anomaly that affects around 1 in 500 women. It accounts for roughly 4–10% of all major uterine anomalies. This disorder arises when one of the Müllerian ducts, which typically create the uterus, does not develop properly or at all [5]. Upto 40% of the women population having a unicornuate uterus also tend to have other urinary system complications such as renal agenesis, which is the absence of kidney on either of the sides [5]. Women who have previous experience of several abortions or prolonged infertility are likely to develop such a condition [5].
Before these diagnoses were officially recorded in the database, there were about 4.74 diagnoses for every 100,000 newborns. The number has remained very stable since 2010, rising to 25.4 per 100,000 [5]. Some tendencies were found when the traits of women with unicornuate uteruses were examined that these ladies typically earned more money, were older, and were Caucasian [7]. In-Vitro Fertilization (IVF), private insurance, and a history of cesarean sections were common. Thyroid issues were also found in a noticeable fraction of the impacted population [7].
When the Müllerian ducts don’t develop correctly during early pregnancy, it can lead to birth defects that affect parts of the female reproductive system—like the uterus, cervix, or vagina. These are known as Müllerian anomalies. The uterus, cervix, and vagina are among the reproductive organs that may be impacted by these anomalies. An estimated 5.5% of the general population is thought to suffer from one of these disorders, and the percentage is roughly 8% higher for women who are infertile. The capacity of a woman to conceive and carry a pregnancy to term can be greatly impacted by these illnesses [6]. Women are often diagnosed with an unicornuate uterus when they seek help for infertility, early pregnancy loss, or complications during pregnancy. It may also be discovered during adolescence when a girl experiences painful periods caused by retrograde menstruation [7]. However, because they end up getting mistaken for their monthly cycle discomfort, a lot of these women do not receive a diagnosis straight away. Women with unicornuate uteruses frequently experience reproductive health problems [7]. Infertile women are more likely to conceive spontaneously, while some women with this illness may become pregnant on their own [7]. However, women with a unicornuate uterus who have a functional uterine cavity have had greater success rates for becoming pregnant with the aid of In Vitro Fertilization (IVF) [7]. Despite this, women with this condition are still considered to be in a high-risk group for pregnancy complications, regardless of how they conceive [7].
Doctors tend to use a variety of tests to confirm and thus identify a unicornuate uterus, including MRI, ultrasound, hysterosalpingography, and, more recently, endoscopy techniques including hysteroscopy and laparoscopy [7]. Specifically for more complicated uterine anomalies, it was shown that MRI provided the most complete and accurate diagnosis [6]. The 3D ultrasound version has been proven to be very effective as they are able to assess the uterine morphology more precisely as well as the blood flow [6]. Hence, when these two devices are used together, they complement each other very effectively, helping us to identify the diseases very accurately as well as leading us to manage the disease more precisely [6].
A unicornuate uterus with a rudimentary horn happens when one side of the Müllerian ducts (which normally form the uterus) doesn’t fully develop. In most women, this rudimentary horn does not connect with the main uterine cavity [8].
A pregnancy in a Noncommunicating Rudimentary Horn (NCRHP) is extremely rare, which has been estimated to be about 1 in 76,000 to 1 in 160,000 pregnancies. Since the cavity doesn’t connect to the main uterus, the pregnancy usually happens because sperm (or sometimes a fertilized egg) travels through the abdominal cavity to reach the rudimentary horn [8]. Unfortunately, these pregnancies are very dangerous. In most cases, the pregnancy cannot be detected early, and the diagnosis is only made after the horn ruptures, often before the third trimester. Rupture can cause massive internal bleeding and hypovolemic shock, making it a life-threatening emergency. Most patients present with abdominal pain, but only about 8% of cases are diagnosed before symptoms appear [8].
If detected early (especially in the first trimester), the pregnancy can be managed safely with laparoscopic surgery to remove the horn. MRI can be very useful in making this diagnosis before complications occur. In some situations, Laparoscopic surgery has even been carried out in the second trimester in certain cases [8].
Transperitoneal migration is the ability of sperm to move across the peritoneal cavity, typically via the Douglas pouch, to reach the ovary or fallopian tube on the other side. This unusual pathway allows fertilization to occur even when the normal route is blocked, and it can sometimes result in ectopic pregnancies or other rare reproductive outcomes.
Transperitoneal migration is regarded as the contributor of ectopic pregnancy [10]. This conclusion is determined on the basis that the corpus luteum is found to be on the contralateral side in about 15-20% of ectopic pregnancy which is considered high. In a 20th-century review of noncommunicating rudimentary horn pregnancies, the data implied that sperm migration through the peritoneal cavity may occur in approximately 48–51% of pregnancies. According to the study done by Nahum GG, Stanislaw H, McMahon C, out of 292 reported pregnancies, 272 occurred in a rudimentary uterine horn, giving a ratio of 0.93 [10]. This suggests that sperm crossing the peritoneal cavity (transperitoneal migration) happens in about 48% of cases. Based on parity distribution, the chance of a rudimentary horn pregnancy per pregnancy was estimated at about 51% (95% CI: 48–56%). In rudimentary horn pregnancies, the migration of sperm across the peritoneal cavity is often regarded as the main reason.
Transperitoneal migration itself does not require treatment, but when it results in conditions like ectopic pregnancy or rudimentary horn pregnancy, management follows standard protocols, which include early diagnosis, surgical removal such as salpingectomy or salpingotomy, methotrexate in selected ectopic cases, and close follow-up.
This case study exposes a rare occurrence of fertilization in a non-communicating right rudimentary horn uterus through transperitoneal passage of sperm. However, a complex obstetric care plan focusing on non-invasive procedures and hormonal therapy successfully mitigates the patient’s chronic infertility.
Conflicts of interest: There are no conflicts of interest.
Acknowledgments: We thank the authors for their valuable contribution to this project.
