1Department of Occupational Therapy, Faculty of Health Sciences, University of Western Macedonia, Ptolemaida, Greece.
2Department of Neurology, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece.
3Department of Psychiatry, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece.
4Greek Association of Alzheimer’s Disease and Related Disorders, Thessaloniki, Greece.
Bourakis Ioannis
Email: gmpourakis@yahoo.gr
Received : Jul 01, 2025 Accepted : Aug 20, 2025 Published : Aug 27, 2025 Archived : www.meddiscoveries.org
Background: Taste and olfactory dysfunction can be useful tools for the early diagnosis of Alzheimer’s (AD) and Parkinson’s (PD) diseases. Although they have been described as early symptoms of the aforementioned diseases in the international literature, whether they can be considered precursor biomarkers has not been sufficiently clarified.
Objective: The present study aims to investigate the apparent correlation between olfactory and gustatory impairment and the clinical signs of AD and PD, through a systematic review of the current literature.
Methods: A systematic review was conducted in the Medline (Pubmed) and Cochrane Central Register of Controlled Trials (Central) databases from January 2020 to February 2023. Longitudinal clinical trials conducted in people with either AD or PD as well as simultaneously examined for olfactory and/or gustatory impairment. The quality of the evidence was assessed using the Rob-2, Cochrane risk of bias tool.
Results: Among 7,760 articles identified, ten longitudinal research studies met the clearly defined criteria and were submitted to extract specific information. 6 clinical trials for MCI, 4 AD and 4 PD were identified.
Conclusions: The sense of smell and taste appeared to decrease to a maximum extent several years before the onset of symptoms of AD and PD. It is of utmost importance that more experimental studies, ideally with a low risk of bias, are needed to record the thresholds of smell and taste in both healthy elderly and people with AD and PD.
Keywords: Hyposmia; Anosmia; Ageusia; Hypogeusia; Parkinson’s disease; Alzheimer’s disease.
It is well known that dementia, as a major and global public health phenomenon, includes, many forms but the two most important forms, are that of Alzheimer’s Disease (AD) and that of Parkinson’s Disease (PD) [1-3].
More specifically, AD was first described by Alois Alzheimer (1907) as a progressive neurodegenerative disease. It affects more than 55 million people worldwide, with a ratio of 1,6:1 (female: male) [4-8] and with increasing prevalence (35%) by 2050 [6-7,9-12]. In the initial stages, it is characterized, clinically, by the appearance of memory and other cognitive deficits [3,7,12-13] through the detection of abnormally folded proteins pathologically (Aβ: β-amyloid and hyperphosphorylated tau) [3,6-8,11,12,14,15]. Additionally, it is important to mention that no effective treatment has been discovered so far.
In contrast, PD was first reported by James Parkinson (1817) as a progressive neurodegenerative disorder [16-19]. Indeed, PD may progress to dementia but is typically classified as a movement disorder. More specifically, it is estimated to affect 6.1 million people worldwide, with a ratio of 3:2 (male: female), and is expected to increase further by the end of 2030 [19-22]. Furthermore, its semiology is distinguished into motor (rigidity, bradykinesia, tremor, inability to make compensatory movements) and non-motor characteristics (dysfunction of the gustatory & olfactory system, sleep, autonomic regulation, neuropsychiatric deficits) [19,21,23-25]. At the same time, the above clinical symptoms are due to the selective degeneration of both dopaminergic neurons in the substantia nigra of the brainstem and of the impending dopaminergic deficit in the striatum [16,20,22,25]. In addition, the absence of a therapeutic regimen for this neurodegenerative disease should be emphasized.
It is commonly accepted that the sense of smell is of crucial importance for the daily survival of people. This happens because on the one side, it is a protective mechanism against exogenous environmental factors and on the other side it is responsible for examining edible products and social communication [9,26,27]. Anatomically, it is divided into the peripheral (detection-processing-transmission of small parts of odors through sensory receptors-formation of the olfactory pathway) and the central olfactory system (primary-secondary olfactory cortex) [8,28-30].
It is commonly accepted that the sense of smell is of crucial importance for the daily survival of people. This happens because on the one side, it is a protective mechanism against exogenous environmental factors and on the other side it is responsible for examining edible products and social communication [9,26,27]. Anatomically, it is divided into the peripheral (detection-processing-transmission of small parts of odors through sensory receptors-formation of the olfactory pathway) and the central olfactory system (primary-secondary olfactory cortex) [8,28-30].
Taste disturbances in alzheimer’s disease
It is known that, in AD, the normal function of taste is disrupted resulting in taste disturbances. In particular, the frequently presented types are dysgeusia, namely alterations in the aesthetic perception of the taste stimulus, and phantogeusia or an unpleasant taste due to taste illusions [30,33]. At the same time, in the later stages of the disease, dysphagia of the oral stage was observed. In other words, it was characterized by reduced tongue motility, prolonged chewing of food, delayed swallowing and increased feeding duration [13]. More specifically, as neurodegeneration progressed, dysphagia symptoms (residues, coughing, choking) worsened. These, in turn, could lead to either poor quality of life (malnutrition, dehydration, poor oral hygiene, missing teeth) or death (aspiration, pneumonia) [13,34-35]. Optionally, it is worth noting that patients did not have self-awareness of pain due to their impaired cognitive background [34].
Olfactory disturbances in alzheimer’s disease
There is no doubt that patients with AD presented clinically pathological findings in the olfactory system. In this case, the presence of hyposmia, as a reduced olfactory ability, and anosmia, namely absence of a functional sense of smell, were likely to be visible for a long period up to years before cognitive symptoms [2,4,8,28]. In addition, recent studies have demonstrated olfactory dysfunctions in odor threshold, recognition, discrimination and memory [1,2,8,12,15,26,28,36]. Furthermore, it is noteworthy to mention on the one side the effect of the emotional state and consequently the reduction of the quality of life and on the other side the inability to know the aforementioned disorder [9,35]. For the above reasons, olfactory disturbances could be a primary predictor of AD onset, severity or progression [1,2,8,12,26,28,36].
Taste disturbances in Parkinson’s disease
It is a fact that disorders of the gustatory system in PD have been investigated in greater depth compared to AD. Based on this position, according to some research, hypogeusia was recorded, and namely reduction of taste perception (back third of the tongue, VII, IX) of salty, sweet or bitter stimuli. In contrast, other studies emphasized ageusia, as the absence of functional taste, with ambiguous conclusions about the time elapsed before (2-10 years) or after diagnosis [30,32,37]. In addition, “frozen” facial expression (bradykinesia), swallowing disorder (muscle rigidity), orofacial dyskinesia and dystonia were observed [16,24,37]. Additionally, patients had difficulty masticating due to the onset of tremors and stiffness in orofacial muscles (tongue, lips) [16,24,37,38]. This resulted in both severe discomfort due to pain (temporomandibular joint, grinding & tooth breakage) as well as poor nutritional quality, malnutrition (inability to control bolus, slow tongue movement & mastication) and low quality of life [23,37-39]. It could be pointed out that oral health requires attention in PD, given either dry mouth (caries, periodontitis) or excessive salivation, as a result of the drugs taken to delay its symptoms [16,19-20,24,37].
Olfactory disorders in parkinson’s disease
By consensus, 90% of people with PD showed disturbances in the olfactory system [25,28,30,40]. In this case, hyposmia, namely reduced olfactory perception and anosmia, as a complete inability to smell, were likely to be diagnosed 4-6 years before the presence of the motor signs of the disease [21,28,30,32]. Also, olfactory deficits referred to the localization, differentiation, identification and recognition of olfactory stimuli, with a greater frequency in the male sex [25,28,30,32,40-41]. In conclusion, it is necessary to emphasize that many studies have argued that the early detection of olfactory dysfunction could be an important biomarker for PD but also for its differential diagnosis from other subtypes of Parkinsonism [21,25,28,30,32,40-41].
Studies examining the effect of olfactory and gustatory dysfunction on AD and PD.
Studies examining the effect of olfactory and gustatory dysfunction on AD and PD.
Few and varied studies have been conducted on the impact of olfactory and gustatory pathology in AD and PD. Initially, Martínez et al. (2018) conducted a review to demonstrate the valuable clinical role of olfaction as a biomarker for both healthy elderly and individuals with neurodegenerative disorders (AD, PD, epilepsy). More specifically, it was pointed out that olfactory function changes with age, as a result of typical aging, altering the localization, detection and discrimination of olfactory stimuli at various levels. In contrast, in humans with AD, clinical diagnosis should be based on olfactory identification. However, identification and olfactory threshold tests are the main focuses of clinical assessment for older adults with PD.
Winchester & Martyn (2020) conducted a systematic review to examine whether the olfactory test can predict cognitive ability in people with AD. In particular, it was shown that the pathology of the sense of smell is strongly related to the impairment of cognitive function. However, they did not account for the influence of important variables (head trauma, smoking, respiratory tract infection) and the use of an inappropriate olfactory test. Nevertheless, it was confirmed that olfactory dysfunction is a predictive factor for late-life cognitive impairment, although the improvement of the olfactory test is expected to be ascertained in future research.
At the same time, Rebholz et al. (2020) performed a review to describe anosmia and aguesia as early biomarkers in both PD and AD as well as in non-neurodegenerative diseases such as SARS-CoV2.
Then, Melis et al. (2021) studied, through their review, the effect of risk factors (molecular & genetic) on taste and smell dysfunction, occurring in PD disease and their relationship with the microbiota. More specifically, it was found impossible to determine the relevant influencing factors of the aforementioned mechanisms of gustatory and olfactory pathology in PD disease due to insufficient data. However, a strong correlation was observed between the senses of smell and taste in people with PD. In this way, they confirmed that their deficits can be characterized as early non-motor symptoms of the aforementioned disease. Furthermore, they supported the predictive value of the above pathologies in the diagnostic definition of PD disease. The olfactory dysfunction is due to the accumulation of α-synuclein, while the taste dysfunction is due to the involvement of the cortex.
Finally, Petekkaya et al. (2022) conducted a study on the observed brain volume changes, in PD and AD subjects, with a dysfunctional olfactory & gustatory system, through the administration of endocannabinoids. In particular, they concluded that on the one side brain alterations are found in the gustatory and olfactory parts of people with PD and AD and on the other hand endocannabinoids significantly contributed to brain volume changes as well as the affected sensory system.
Given the significant role of the contribution of olfactory and gustatory dysfunction in the early diagnosis of AD and PD diseases and considering the limited number of research studies that have been conducted to date in this field, the purpose of the present review is to collect and record data on with the effect of olfaction and taste impairment in AD and PD. More specifically, this paper will conduct a systematic review of the incidence, diagnostic tools, sex, age and factors of olfactory and gustatory impairment in AD and PD.
Purpose of the study
The purpose of this research is to investigate the correlation of olfactory and gustatory dysfunction in adults (age > 18) with AD and PD. In order to achieve the higher purpose, the following research questions are formulated:
1: What is the prevalence of olfactory dysfunction in people with AD and PD?
2: What is the prevalence rate of taste dysfunction in people with AD and PD?
3: What are the factors of olfactory dysfunction affecting people with AD and PD?
4: What are the factors of taste dysfunction affecting people with AD and PD?
Search strategy
First, a systematic search was conducted on January 1st, 2020 to detect the studies, which refer to the association of olfactory and gustatory dysfunction with AD and PD. In addition, the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines were followed. More specifically, the search was conducted using the academic databases (Medline – Pubmed, Cochrane Central Register of Controlled Trials – Central) through the folfollowing keywords: “evaluation” or “risk factors” or “biomarkers” or “loss of taste” or “loss of smell” or “dysfunction of gustatory” or “dysfunction of olfactory” or “anosmia” or “hyposmia” or “dysosmia” or “hypogeysia” or “ageusia” or “dysgeusia” or “olfactory impairment” or “gustatory impairment” or “odor detection threshold tests” or “odor identification threshold tests” or “odor discrimination tests” or “odor intensity tests” or “taste tests” or “chemical threshold tests” or “electrical threshold tests” or “taste identification tests” or “taste intensity tests” or “Parkinson” or “Alzheimer” or “Mild Cognitive Impairment” as well as possible combinations between them. Studies were identified by the two authors (IB, MT) up to February 2023. This protocol has not been registered in the PROSPERO.
Eligibility criteria
The inclusion criteria were the following: A) The sample included adult people (age > 18) with AD and PD disease (from mild cognitive impairment to severe dementia). In particular, the type of AD included: 1) Mild Cognitive Impairment (MCI), 2) Mild Dementia, 3) Moderate Dementia and 4) Severe Dementia. On the other side, the type of PD included: 1) Primary Parkinsonism (idiopathic), 2) Familial type of PD, 3) Early-onset type of PD, 4) Atypical Parkinsonism (Dementia with Lewy Bodies, Progressive Supranuclear Palsy, Corticobasal Degeneration, Multiple System Atrophy) and 5) Secondary Parkinsonism (Drug-induced Parkinsonism, Vascular Parkinsonism, Normal Pressure Hydrocephalus, Infections, Toxins, Trauma). B) The included studies were Randomized Controlled Trial (RCT) studies. C) The publication date was for the years 2020-2023. D) The language of publication was English.
The exclusion criteria were the following: A) animal/in vitro studies, case studies, reports, reviews and editorials. B) Studies, which did not concern olfactory and gustatory dysfunction in PD and AD diseases (MCI, Mild, Moderate, Severe Dementia of the AD type). C) Research published before 2020. D) Studies published in another language than English.
Selection criteria and data extraction
Independent data extraction was performed by two researchers (IB, MT) and discrepancies were resolved through discussion with the other authors. In more detail, the following variables were extracted: Study (first author and year of publication), Country, Population (PD, MCI, Mild, Moderate or Severe type of AD), Diagnostic instrument, type of olfactory or taste dysfunction, age, sex as well as factors.
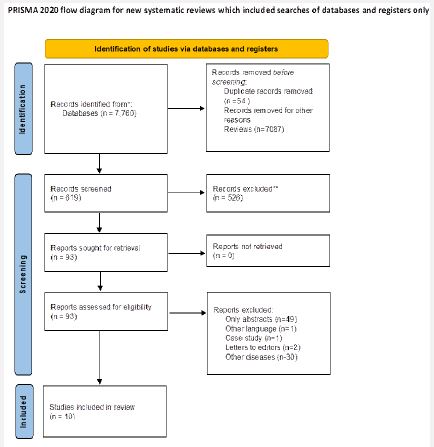
In the first phase, 7,760 relevant results were found. After removing duplicates (n=54) and reviews (n=7087) the remaining 619 articles were analyzed according to the predefined criteria. In particular, the two authors (IB, MT) assessed the title and abstract of the specific studies, through the double-blind method, to clarify whether the inclusion and exclusion criteria were met. After this process, 526 articles were removed, and 93 articles were read in full. Of these, 83 studies were excluded, because 49 studies had only the abstract, 1 article was in Spanish, 2 studies were letters to editors, 1 article was a case study and 30 studies referred to other disorders. Finally, 10 articles were included in this review. The relevant flowchart is shown in Figure 1.
Risk of bias and study quality: The 2 reviewers (IM, MT) independently assessed the risk of bias and the quality of the studies using the quality assessment tool ROB-2, which is provided by Cochrane for the assessment of randomized trials [43]. In detail, it consists of 5 axes (randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result), each of which is scored by answering (Yes, Probably Yes, Probably No, No, No Information) to a series of questions regarding the design, conduct and reporting of the trials. The answers then guide the researcher, through an algorithm, in formulating a judgment (low, high, some concerns).
10 articles were studied, to conclude the effect of olfactory and gustatory dysfunctions in PD and AD diseases. Specifically, the specified investigations were conducted in Italy, Mexico, Russia, Ukraine and Singapore. However, most of the studies came from the United States of America, Japan, and Korea.
All studies were Randomized Controlled Trials (RCT) and are presented in detail in Table 1. More specifically, in each table, the characteristics of the population to be studied are presented, namely whether they are healthy with an increased risk of the previously mentioned diseases or whether they are people diagnosed with PD, MCI or AD. Then, the diagnostic tools used to detect the pathologies of the olfactory and gustatory systems are described. After, the types and percentages of the pathologies of smell and taste are recorded. Then, the age, which varies from 40 to 92 years, and the gender (men: women) are noted. Finally, the factors that contribute to the development of specific diseases are listed. In conclusion, the studies were grouped based on the presenting disease, while the studies on AD were divided into further categories, namely MCI, and dementia.
Correlating the effect of olfactory and gustatory impairments on mild cognitive impairment (MCI)
Smell and taste disorders appear to significantly affect people with MCI. More specifically, six studies were identified, four of which reported on olfactory [47,48,51,52] and the other two [50,53] on taste dysfunction (Table 2).
In particular, one study evaluated the tau tracer [18F]-JNJ-64326067-AAA ([18F]-JNJ-067) in healthy adults, MCI, AD & PSP and observed that only people with MCI & AD were positive for amyloid. However, there was no statistically significant difference between older adults with MCI or PSP and healthy individuals [47].
In a 2-year randomized controlled trial, a positive association of younger age with the target - regions of interest (ROI) but a negative effect on the off-target regions (Off - OTS ROI), a fact that is also proven by other studies with corresponding markers (tau, Aβ, RO948). They also concluded that gender does not influence pathology as much as the size of the meningeal OTS (MK6240), with women dominating. Most important, however, was the interdependence between olfactory and cognitive function, where when the former was impaired in individuals with MCI, then the latter predicted degeneration into AD-like dementia [48].
An interventional diagnostic study highlighted the strong association of olfactory pathology with MCI. Additionally, a strong relationship between olfactory impairment and both cognitive tests (Mini-Mental State Examination-MMSE, Seoul Neuropsychological Screening Battery) and diagnostic classification was reported [51].
In a randomized controlled trial, the frequency of olfactory pathologies in MCI was recorded at 88.6%, without, however, identifying any specific type of olfactory deficit [52].
In a randomized clinical trial, it was verified that tooth loss contributed to the rapid transition from the level of cognitive impairment to that of dementia. Furthermore, it was noted that faster CBF velocity, which decreases with advancing age, was associated with masticatory ability. Consequently, reduced brain function in older adults, combined with poor blood circulation and low CBF velocity, disposed to lead to cognitive decline [50].
In a randomized controlled trial, only women with the non-aMCI subtype, who had received higher education, had reduced levels of Aβ-42 in their saliva [53].
Finally, the risk of bias was high for five studies [47,48,50-52] and one [53] had some concerns.
| Characteristics of included studies | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Article | Year | Country | Population | Diagnostic instrument | Olfactory dysfunction | Gustatory dysfunction | Age | Sex | Another factors |
| Baba et al. | 2022 | Japan | Parkinson | OSIT-J<4 | Severe hyposmia (41%) | 55-75 | M:121 F:80 | severe olfactory function, age, duration of PD, severe motor impairment, posturalinstabil- ity, MCI correlation ofseverity of olfactory dysfunctionwith the degree of cholinergic deficits,Olfactory deficits, REM sleep behav- iourdisorder, orthostatic hypotension, CSF Αβ,GBA mutation, posterior predominant corticalhypometabolism, atrophy in basal forebraincholinergic nucleus | |
| Flores- Silvaet al. | 2021 | Mexico | Covid-19 & 1 Parkinson | CT, MRIor both | Anosmia (7%) | Dysgeusia(8%) | >18 (53+-13) | M:697 F:375 | comorbidity of obesity(43.6%), hypertension (33.7%), diabetes (27.6%), Smoking(12.3%),HIV (2,5%), Pulmonary (5.5%), Cardiovascular(4.9%), Neurologic (12.3%) & Autoimmunedisease (8%) |
| Baker et al. | 2021 | USA | HCs,MCI, AD, PSP | tau-PET, Aβ-PET, structuralMRI scan | 64-92 | M:7 F:10 | detection of pathological forms tau (intrana- sally) that affect cognitive function in AD | ||
| Harrison et al. | 2023 | USA | MCI | tau-PET, Aβ-PET, structural MRI scan, created OTS-ROI | 60-79 | M:162 F:319 | ROI-positive correlation with ageOTSROI -negative correlation with age OTS gender correlation (female) & size (higher) | ||
| Isaacson et al. | 2020 | USA, Rus-sia, Ukraine | Parkinson &Neurological disorders (122 Parkinson) | USFR, CGI-C, CGI-S PGI-C,PGI-S, DFSS-I DFSS-P,DISDental exam | Salivation (74%) | 63.9 (+-13.3) | M:144 F:40 | perioral chapping, excoriation of the skin around the mouth, oral hygiene problems, speech difficulties & sleepinterruption, dental caries &periodontal disease higher in patients with PD (65%)risks: constipation,bradycardia, cognitive enhancement, drowsi-ness, urinary retention, pneumonia, dysfagia, dry mouth | |
| Jung et al. | 2022 | Korea | CN, MCI &Control | GOHAIEEGDental examOHIP-14 | Oral health(teeth, chewing, salivation) | >65 | M:6 F:46 | Aging (reduction CBF & cognitive function) higherlevel of stress,depression Oral Health(chewing disorders, speech dysfunction, mouth pain, tooth loss) | |
| Kim et al. | 2022 | SouthKorea | AD, MCI,normalyounger adults | Olfactory stimulation PET,CT | >60 | M:0 F:168 | correlation of olfactory dysfunction with MCI | ||
| Kouzuki et al. | 2020 | Japan | AD & MCI | OSIT-J | Olfactory dysfunction (88.6%) | 75-84 | M:17 | Drowsiness aging | |
| Ng et al. | 2021 | Singapo re | MCI (aMCI:21,non- aMCI:34) | Salivary Aβ-42 | 60-86 | M:14 F:41 | Cognitive stocksex & typeof MCI | ||
| Takahashiet al. | 2020 | Japan | AD | OSIT-J | Anosmia | Dysgeusia, lossof appetite | Intervention group: 76.2+-9.8Control group: 75.8+-7.8 | M:14 F:22 | aging correlation of olfactory dysfunction & cognitive decline |
OSIT-J: Odor Stick Identification Test for Japanese; PD: Parkinson Disease; MCI: Mild Cognitive Impairment; REM: Rapid Eye Movement, CSF: Cerebrospinal Fluid; Aβ: β-Amyloid Peptide; GBA: β-Glucosylceramidase; AD: Alzheimer Disease; PSP: Progressive Supranuclear Palsy; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; HIV: Human Immunodeficiency Virus; PET: Positron Emission Tomography, OTS: Off – Target Signal; ROI: Region of Interest; USFR: Unstimulated Salivary Flow-Rate; CGI-C: Clinical Global Impression of Change; CGI-S: Clinical Global Impressions of Severity; PGI-C: Patient-Rated Global Impressions of Change; PGI-S: Patient-Rated Global Impressions of Severity; DFSS-I: Drooling Frequency and Severity Scale by Investigator; DFSS-P: Drooling Frequency and Severity Scale by Patient; DIS: Drooling Impact Score; CN: Cognitively Normal; GOHAI: Geriatric Oral Health Assessment Index; EEG: Electroencephalography; OHIP: Oral Health Impact Profile; CBF: Celebral Blood Flow; aMCI: Amnestic Mild Cognitive Impairment; Non-aMCI: Non-Amnestic Mild Cognitive Impairment.
| Characteristics of included studies | MCI | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Article | Year | Country | Population | Diagnostic Instrument | Olfactory dysfunction | Gustatory dysfunction | Age | Sex | Another Factors |
| Baker et al. | 2021 | USA | HCs, MCI, AD, PSP | tau-PET, Aβ-PET,structural MRI scan | 64-92 | M:7 F:10 | Detection of pathological formstau (intranasally) that affect cognitive function in AD | ||
| Harrison et al. | 2023 | USA | MCI | tau-PET, Aβ-PET,structural MRI scan, created OTS-ROI | 60-79 | M:162 F:319 | ROI-positive correlation with ageOTS ROI -negative correlation with ageOTS gendercorrelation (female) &size (higher) | ||
| Jung et al. | 2022 | Korea | CN, MCI &Control | GOHAIEEGDental exam OHIP-14 | Oral health(teeth, chewing, salivation) | >65 | M:6 F:46 | Aging (reduction CBF & cognitive function) higher level of stress, depression Oral Health(chewing disorders, speechdysfunction, mouth pain,tooth loss) | |
| Kim et al. | 2022 | SouthKorea | AD, MCI,normal youngeradults | Olfactory stimulation PET, CT | >60 | M:0 F:168 | Correlation of olfactory dysfunction with MCI | ||
| Kouzukiet al. | 2020 | Japan | AD & MCI | OSIT-J | Olfactory dysfunction (88.6%) | 75-84 | M:17 F:18 | Drowsiness aging | |
| Ng et al. | 2021 | Singapore | MCI (aMCI: 21,non-aMCI:34) | Salivary Aβ-42 | 60-86 | M:14 F:41 | Cognitive stocksex & typeof MCI | ||
OSIT-J: Odor Stick Identification Test for Japanese, MCI: Mild Cognitive Impairment, Aβ: β-Amyloid peptide, AD: Alzheimer Disease, PSP: Progressive Supranuclear Palsy, CT: Computed Tomography, MRI: Magnetic Resonance Imaging, PET: Positron Emission Tomography, OTS: Off – Target Signal, ROI: Region of Interest, CN: Cognitively Normal, GOHAI: Geriatric Oral Health Assessment Index, EEG: Electroencephalography, OHIP: Oral Health Impact Profile, CBF: Celebral Blood Flow, aMCI: amnestic Mild Cognitive Impairment, non-aMCI: non-amnestic Mild Cognitive Impairment.
Correlating the effect of olfactory and gustatory dysfunctions on AD
On the opposite side, four studies were found on the impact of olfactory and gustatory dysfunctions in people with AD. Specifically, three studies were detected on olfactory [47,51,52] and one [54] on gustatory pathology (Table 3).
More specifically, one study evaluated the tau tracer [18F]-JNJ-64326067-AAA ([18F]-JNJ-067) in healthy adults, MCI, AD & PSP and observed that only people with MCI & AD were positive for amyloid. However, only individuals with AD showed an increased percentage of this particular tracer, in most areas of the olfactory cortex, compared to older adults without cognitive difficulties. Furthermore, in the temporal lobe and olfactory bulb region, a strong correlation was shown between the aforementioned tracer and the diagnostic tool MMSE [47].
Similar results were also reported in an interventional diagnostic study, which highlighted the strong relationship between olfactory impairment with both cognitive tests (MMSE, Seoul Neuropsychological Screening Battery) and with the diagnostic accuracy of the classification [51].
In a randomized controlled trial, the frequency of olfactory pathologies in AD was recorded at 88.6%, without, however, identifying any specific type of olfactory deficit. Furthermore, no significant statistical conclusions were noted except for the association of sleep function with that of cognition, after the use of aromatic salt during bathing [52].
In a clinical trial, the prevalence of taste disorders was not determined but dysgeusia and loss of appetite were noted. In addition, a statistically significant difference was found between the Neuropsychiatric Inventory (NPI) and the Japanese version of the Zarit Caregiver Burden Interview (J-ZBI), clarifying the reduction of psychological and behavioral symptoms as well as the workload of caregivers [54].
Finally, the risk of bias was high for all studies [47,51,52,54].
| Characteris tics of included studies | AD | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Article | Year | Place | Population | Diagnostic Instrument | Olfactory dysfunction | Gustatory dysfunction | Age | Sex | Another factors |
| Baker et al. | 2021 | USA | HCs,MCI, AD, PSP | tau-PET, Aβ- PET, structural MRI scan | 64-92 | M:7 F:10 | Detection of pathological forms tau (intranasally) that affectcognitive function in AD | ||
| Kim et al. | 2022 | SouthKorea | AD, MCI,normalyounger adults | Olfactory stimulation PET, CT | >60 | M:0 F:168 | Correlation of olfactory dysfunction with MCI | ||
| Kouzukiet al. | 2020 | Japan | AD &MCI | OSIT-J | Olfactory dysfunction (88.6%) | 75-84 | M:17 F:18 | Drowsiness aging | |
| Takahashiet al. | 2020 | Japan | AD | OSIT-J | Anosmia | Dysgeusia, loss of appetite | Intervention group:76.2±9.8 Controlgroup: 75.8±7.8 | M:14 F:22 | Aging correlation of olfactory dysfunction & cognitivedecline |
OSIT-J: Odor Stick Identification Test for Japanese; MCI: Mild Cognitive Impairment, Aβ: β-Amyloid Peptide; AD: Alzheimer Disease; PSP: Progressive Supranuclear Palsy; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; PET: Positron Emission Tomography; CN: Cognitively Normal; aMCI: amnestic Mild Cognitive Impairment; Non-aMCI: Non-amnestic Mild Cognitive Impairment.
Correlating the impact of olfactory and gustatory dysfunctions in PD
In contrast, four studies were identified regarding the impact of olfactory and gustatory dysfunctions in people with PD. Indeed, PD may progress to dementia but is typically classified as a movement disorder. Specifically, three studies were identified regarding olfactory [45-47,51] and two [46,49] regarding gustatory pathology (Table 3).
More specifically, in a multicenter, double-blind, randomized trial in non-demented PD people with severe hyposmia, the prevalence of olfactory disorders was recorded, on average, at 41.7%, with severe hyposmia being the main manifestation. Furthermore, the most important factors for the progression of PD to Parkinson’s Disease Dementia (PDD) were found to be older age, postural instability, mild cognitive impairment, and severe motor impairment. In addition, non-motor symptoms (olfactory dysfunction, rapid eye movement-REM sleep disorder, orthostatic hypotension), CSF Aβ, the GBA gene, vascular lesions (cholinergic nucleus atrophy), and cortical hypometabolism could be added [45].
In a prospective, cross-sectional observational study conducted at the Salvador Zubiran National Institute of Medicine and Nutrition, it was noted that the prevalence of olfactory pathologies was 7%, with the occurrence of anosmia, although the frequency of gustatory dysfunction was 8% with the presence of dysgeusia. In addition, for the pathogenesis of both PD and other neurological manifestations, obesity (43.6%), hypertension (33.7%), diabetes (27.6%), and smoking (12.3%) played a decisive role. In addition, the above factors included neurological diseases (12.3%), autoimmune (8%) and cardiovascular (4.9%) disorders, lung disorder (5.5%) as well as human immunodeficiency virus (HIV) infection (2.5%) [46].
and Nutrition, it was noted that the prevalence of olfactory pathologies was 7%, with the occurrence of anosmia, although the frequency of gustatory dysfunction was 8% with the presence of dysgeusia. In addition, for the pathogenesis of both PD and other neurological manifestations, obesity (43.6%), hypertension (33.7%), diabetes (27.6%), and smoking (12.3%) played a decisive role. In addition, the above factors included neurological diseases (12.3%), autoimmune (8%) and cardiovascular (4.9%) disorders, lung disorder (5.5%) as well as human immunodeficiency virus (HIV) infection (2.5%) [46].
In a randomized, parallel, double-blind, controlled clinical trial, it was found that individuals with PD are at high risk of developing drooling, at a rate of 74%. It was also noted that high salivation frequency can lead to various perioral problems (cracking, dermatitis), oral hygiene difficulties, development of speech problems and sleep disturbance. In conclusion, pharmacological treatment of saliva was likely to cause additional side effects such as dry mouth, dysphagia, caries, periodontal disease (65%), pneumonia, constipation, bradycardia, cognitive impairment, drowsiness and urinary retention [49].
Finally, the risk of bias was high for one study [47], some concerns for two [46,49] and low for one [45].
Risk of bias and study quality
The results of the ROB-2 assessment tool showed that the average of the studies was High, which suggests that the methodological quality of the randomized clinical trials included in this review was not generally good. Specifically, according to the ROB-2 algorithm, six studies were High, three Some Concerns and one Low (Table 5).
| Characteristics of included studies | PD | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Article | Year | Country | Population | Diagnostic Instrument | Olfactory dysfunction | Gustatory dysfunction | Age | Sex | Another Factors |
| Baba et al. | 2022 | Japan | Parkinson | OSIT-J<4 | Severe hy- posmia(41%) | 55-75 | M:121 F:80 | Severeolfactory function, age, duration of PD, severe motor impair- ment, postural instability, MCIcorrelation of severity of olfactory dysfunction withthe degree of cholinergic deficits, Olfactory deficits, REM sleep behaviour disorder, orthostatic hypotension, CSF Αβ, GBA mutation,posterior predominant cortical hypometabolism, atrophy in basal forebrain cholinergic nucleus | |
| Flores- Silva et al. | 2021 | Mexico | Covid-19 & 1 Parkinson | CT, MRI orboth | Anosmia (7%) | Dysgeusia(8%) | >18(53+-13) | M:697 F:375 | Comorbidity of obesity (43.6%), hypertension (33.7%), diabetes (27.6%), Smoking (12.3%), HIV (2,5%), Pulmonary (5.5%), Cardiovas-cular (4.9%), Neurologic (12.3%) & Autoimmune disease(8%) |
| Baker et al. | 2021 | USA | HCs, MCI, AD, PSP | tau-PET, Aβ-PET,structuralMRI scan | 64-92 | M:7 F:10 | Detection of pathological forms tau (intranasally) that affect cognitive function in AD | ||
| Isaacson et al. | 2020 | USA, Russia, | Parkinson & Neuro-logical dis- orders (122 Parkinson) | USFR, CGI- C, CGI-S | Salivation (74%) | 63.9 (+-13.3) | M:144 | Perioral chapping,excoriation of the skin around the mouth,oral hy- giene problems, speechdifficulties & sleepinterruption, dental caries& periodontal disease higher in patients with PD (65%) | |
| Ukraine | PGI-C, PGI- S, DFSS-I DFSS-P, DISDentalexam | F:40 | Risks: constipation, bradycardia, cognitive enhancement, drowsiness, urinary retention, pneumonia, dysfagia, dry mouth | ||||||
OSIT-J: Odor Stick identification Test for Japanese; PD: Parkinson Disease; MCI: Mild Cognitive Impairment; REM: Rapid Eye Movement; CSF: Cerebrospinal Fluid; Aβ: β-Amyloid Peptide; GBA: β-Glucosylceramidase; AD: Alzheimer Disease; PSP: Progressive Supranuclear Palsy; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; HIV: Human Immunodeficiency Virus; PET: Positron Emission Tomography; USFR: Unstimulated Salivary Flow-Rate; CGI-C: Clinical Global Impression of Change; CGI-S: Clinical Global Impressions of Severity; PGI-C: Patient-Rated Global Impressions of Change; PGI-S: Patient-Rated Global Impressions of Severity; DFSS-I: Drooling Frequency and Severity Scale by Investigator; DFSS-P: Drooling Frequency and Severity Scale by Patient; DIS: Drooling Impact Score; CN: Cognitively Normal.
| Study | D1a | D1b | D2a | D2 | D3 | D4 | D5 | Overall |
|---|---|---|---|---|---|---|---|---|
| Baba et al. 2022 | Low | Low | Low | Low | Low | Low | Low | Low |
| Flores- Silvaet al. 2021 | Low | Some concerns | Some concerns | Someconcerns | Low | Low | Low | Some concerns |
| Baker et al. 2021 | High | Low | High | Someconcerns | Low | High | Low | High |
| Harrison et al. 2023 | High | Low | Low | Someconcerns | Low | High | Low | High |
| Isaacson et al. 2020 | Low | Some concerns | Low | Low | Low | Low | Low | Some concerns |
| Jung et al. 2022 | High | Low | Some concerns | Someconcerns | Low | High | Low | High |
| Kim et al. 2022 | High | Low | Low | Someconcerns | Low | High | Low | High |
| Kouzuki et al. 2020 | High | Some concerns | High | Someconcerns | Low | Some concerns | Someconcerns | High |
| Ng et al. 2021 | Low | Low | Low | Someconcerns | Low | Low | Low | Some concerns |
| Takahashi et al. 2020 | High | Low | Low | Someconcerns | Low | High | Low | High |
The early detection of smell and taste disorders is of utmost importance, that could be important biomarkers for the onset of AD and PD diseases [28,33,55-56]. To date, the association of olfactory and gustatory dysfunction in AD and PD has not been examined in detail. In addition, most clinical studies focus on the single finding of olfactory impairment, most often in PD and less often in AD (MCI, AD). Consequently, the present research aimed to examine the data in the literature regarding the connection between olfactory and gustatory pathologies in AD and PD diseases, summarizing the conclusions of longitudinal studies that investigated olfactory and gustatory impairment in individuals with AD and PD.
So, anyone could easily conclude that, according to the data in the literature, AD and PD diseases are included in the most frequent clinical syndromes of dementia. On the opposite side, the senses of taste and smell play a very important role in the daily survival of people. In particular, gustatory and olfactory dysfunction could be useful tools for the early diagnosis of PD and AD, given on the one hand their early decline, ranging from 5-20 years earlier, and on the other hand their high prevalence in the aforementioned diseases. However, olfactory impairment has been sufficiently analyzed to include it in the diagnostic criteria of PD. Also, efforts are emerging for its usefulness in the differential diagnosis, between the subtypes, of specific neurodegenerative diseases. However, taste loss, according to the results of the present review, presented high epidemiological data, which one should consider in the diagnostic process of AD and PD diseases. After all, these 2 senses are connected and interact accordingly with, even though they are distinguished as separate systems and convey information through different nerves.
The specific research papers were selected because they involved people diagnosed with either AD (MCI, mild, moderate & severe AD) or PD. At the same time, they should show olfactory or taste dysfunction.
The most important conclusions of this review could include the fact that gender, in people with MCI, played a decisive role. In this case, the female population (408) was twice as large as the male population (197) [47,48,50-53].
Furthermore, most researchers agreed that age, which ranged from 60-92 years, was a major factor in the age-related decline in olfactory function, which resulted in both a reduced rate of nerve cell regeneration [50,52,48] and the interactive relationship of the latter with cognitive function [53,50,52,48]. This finding was confirmed by a recent study by Harisson et al. (2023), who showed a strong relationship of olfaction with age but not with cognitive function.
A little earlier, Kouzuki et al. (2020) claimed that a negative correlation was found between cognitive, olfactory and sleep function through aromatherapy. However, although no statistically significant differences were noted between the selected trials, the increasing effect of sleep enhancement on cognitive function was commented on. In contrast, she stated that her research contradicts the results of two other studies, which showed that the amount of amyloid β protein in the cerebrospinal fluid showed daily fluctuations (increase-awake, decrease-sleep) and that, in a longitudinal study (3 years) sleep deprivation and sleepiness were considered risk factors for dementia [52].
Also, only one study found that depression and anxiety were identified as notable causes of cognitive decline. In the case of depression, when cognitive decline was observed either in the elderly or in people with MCI, then its effect caused a decrease in mental functions, through neurochemical changes. In the case of anxiety, when detected in high rates, it was then associated with increased weakness of both body and mind. In summary, it is appropriate to emphasize that increased physical stress was due to the existence of tension and unsatisfactory sleep while greater mental stress arose as a result of nervousness and unstable emotional load [50].
The most crucial, however, which was discussed in one of the six studies, was the interdependence between olfactory function and cognitive function, where when the former was impaired in people with MCI, then the latter predicted degeneration into AD-like dementia [51].
The role that cognitive reserve and individual education could play was also important, which was analyzed in a randomized clinical trial [53].
Additionally, it should be noted that only one study included MCI subtypes [53] while only 2 studies investigated the pure MCI population [53,48]. In addition, three studies included control groups [51,50,47], three compared individuals with MCI and AD [47,51,52], while only one showed an association with a different pathology (PSP) [47].
In conclusion, it is worth noting that four randomized clinical trials were conducted on olfactory dysfunction [47,51,52,48], of which only one reported a prevalence rate for this disorder [52] while only two studies on taste pathology [50,53], without reporting a specific degree of its prevalence. Furthermore, the types of disorders in both olfactory and taste function were not noted. More clinical trials are expected to be conducted to clarify the association of olfactory and taste impairment in MCI. Finally, the risk of bias was high for five studies [47,48,50-52] and one [53] had some concerns.
On the contrary, in the case of people with AD, many would agree that age, which ranged from 60 to 92 years, was the most important factor for olfactory dysfunction, since like all senses (e.g. vision, hearing) in the same way, olfactory function begins to decline during old age [52,54].
All studies included in their sample a greater number of women (almost four times) compared to men, which comes to an agreement with the abundance of scientific research on AD disease, which seems to prefer the female gender [47,51,52,54].
Additionally, it has been suggested that olfactory dysfunction could be used as a tool for either early diagnosis or differential diagnosis of AD. This arose from the fact that olfactory pathology was observed in adults with AD, well before cognitive decline and the rapid progression of people with MCI to AD, with worsening olfactory impairment. This notion was confirmed both by the research study of Kim et al. (2022), which used infrared signals in the prefrontal lobe, where olfactory recognition information arrives and by that of Baker et al. (2021), which argued that the tracer [18F]-JNJ-067 was distinguished by its ability to detect pathological tau patterns that had affected the cognitive function of individuals with AD.
In addition, one of the four studies found a high degree of reliability in the classification of individual levels of AD disease, while two found a high correlation between olfactory function and cognitive tests [47,51]. Baker et al. (2021) also reached the same conclusion but with a smaller sample size compared to the previous study. More specifically, they performed scans (PET Aβ, PET tau) to demonstrate that amyloid was detected only in individuals with MCI and AD compared to neurotypicals as well as in individuals diagnosed with PSP. Furthermore, it was noted that only people with AD showed an accumulated amount of amyloid in the nasal cortex. Furthermore, the association of the tau tracer [18F]-JNJ-067 with the Mini-Mental State Examination was recorded in the nasal cortex and temporal lobe regions. Therefore, it was found that [18F]-JNJ-067, which was associated with AD disease, showed no relationship in normal individuals as well as in people with MCI and PSP, due to undetectability of low levels of tau [47].
During the review, a strong association between olfactory functions, sleep, cognition, behavior, as well as psychological symptoms of AD was revealed in 3 studies. All the aforementioned data were verified by Kouzuki et al. (2020), who agreed with Kim et al. (2022) on the interdependent relationship that has been established between cognitive, olfactory and sleep function. However, they failed to demonstrate the improvement of the aforementioned mechanisms through aromatherapy. In contrast, Takahashi et al. (2020) concluded that people with AD (mild, moderate and severe AD) and olfactory stimulation but without olfactory pathology showed a reduction in their behavioral and psychological symptoms after exposure to cedar wood.
Additionally, it should be noted that only one study included the subtypes of AD (mild & moderate) [51] and only one investigated a pure AD population [54]. In addition, two studies included control groups [51,47], three compared individuals with MCI and AD [47,51,52], while only one showed an association with a different pathology (PSP) [47].
Consequently, it is worth noting that four randomized clinical trials were conducted on olfactory dysfunction [47,51,52,54], of which only one reported a prevalence rate for this disorder [52], while only one study on taste pathology [54], without reporting a specific degree of its prevalence. However, only one study [54] noted the types of disorders in both the function of smell (anosmia) and taste (dysgeusia, loss of appetite). More clinical trials are expected to clarify the correlation between olfactory and gustatory impairment in AD. Finally, the risk of bias was high for all studies [47,51,52,54].
In contrast, in the case of people with PD, most researchers would agree that the age range, which ranged from 53 to 92 years, showed an increase in its range, compared to that of MCI and AD participants [45-47,49].
In three of the four studies in this review, the male population was several times larger than the female population, which is consistent with the abundance of scientific research on PD, which seems to favor the male gender [45,46,49].
This review showed that olfactory pathology could be an important predictor of cognitive decline in people with PD. This conclusion was confirmed by the recent study by Baba et al. (2022), who demonstrated that early administration of donepezil to individuals with PD and severe olfactory dysfunction improved their cognitive performance in neuropsychological tests (ACE-R, CDR). However, there was no statistically significant change in the periodicity of the presence of cognitive impairment during a 4-year follow-up with a 6-month assessment in a large sample size (201 people with hyposmia). Similar findings were reached by Flores-Silva et al. (2021), who attempted to capture the characteristics and prognostic indicators that contribute to the occurrence of neurological disorders in people with COVID-19, during their hospitalization. Considering the results of their study, it was found that a person with pre-existing PD presented dysgeusia (8%) and anosmia (7%) among the most common symptoms. Furthermore, it was emphasized that headache, previous neurological disease, mechanical ventilation support and neutrophil/lymphocyte equivalence were considered the main early indicators of in-hospital development of neurological disease.
Regarding taste dysfunction, it was observed that drooling is the most common feature of people with PD. Furthermore, it is considered of utmost importance to emphasize the fact that both its high prevalence (74%) and its drug treatment could bring many side effects such as pneumonia, oral hygiene difficulties, speech problems, skin diseases and sleep disruption. These findings were verified by Isaacson et al. (2020), who claimed that injectable RimabotulinumtoxinB (RIMA) was more effective (1-13 weeks of treatment) than anticholinergic drugs in reducing drooling in a satisfactory sample (122) of people with PD. However, side effects were observed to include dysphagia, caries, and mild to moderate dry mouth.
Additionally, it should be noted that no study included PD subtypes and only one investigated a pure PD population [45]. In addition, one study included a control group [47], three compared individuals with PD, MCI, AD, PSP, Covid-19 and other neurological disorders (diabetes, epilepsy, stroke, migraine, multiple sclerosis, ALS, cerebral palsy) [47,46,49] while three demonstrated an association with a different pathology [47,46,49].
Therefore, it is appropriate to emphasize that three randomized clinical trials were conducted on olfactory dysfunction [45-47], of which two reported a prevalence rate for this disorder [46,45] while two studies on taste pathology [46,49], with the accompanying report of its prevalence rate. However, in three studies [45,46,49] the types of disorders in both the function of smell (anosmia, severe hyposmia) and taste (dysgeusia, drooling) were noted. More clinical trials are expected to clarify the correlation of olfactory and taste impairment in PD. Finally, the risk of bias was high for one study [47], some concerns for two [46, 49] and low for one [45].
It is necessary to point out that the limitations of this study included the search for studies, which was carried out from specific databases such as Medline (Pubmed) and Cochrane Central Register of Controlled Trials (Central). Another limitation of this review was the heterogeneity of studies (duration and type of disease, clinical characteristics of people, assessment tools, and follow-up time). Additionally, dissimilarity was observed in the methodology used to identify olfactory and gustatory impairment. Furthermore, the fact of the different subtypes of each disease should be emphasized, which probably differentiated the final form of the olfactory and gustatory pathology. In conclusion, the insufficiency of longitudinal data regarding the active activity of smell and taste both in neurotypical individuals and in patients with other neurological disorders has been the biggest limitation for the overall picture of the functioning of the specific senses in AD and PD diseases. At the same time, a future study would be legitimate to collect research from more and different databases. At the same time, to incorporate research papers published before 2020. Also, to perform the search with different keywords and in different types of dementia. Therefore, to identify studies, with additional information and with low risk of bias, on olfactory and gustatory impairment in AD and PD in correlation with CSF or blood biomarkers of people with these diseases.
Finally, it is of the utmost importance that more research is needed, to record the thresholds of smell and taste both in healthy elderly people and in those with AD and PD disease, so that it becomes possible to use them, as biomarkers, in modern scientific everyday life.
Conflicts of interest: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Marina Makri is an Associate Editor of the Journal of Alzheimer’s Disease and an Associate Editor of JAD Reports, but was not involved in the peer-review process of this article nor had access to any information regarding its peer review.
Data availability statement: The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Other information: This review has not been registered. No protocol has been prepared. No sources of financial support for the review were found. There are no competing interests among the authors. When published, this review will be available to all in the library of the Department of Medicine of the Aristotle University of Thessaloniki.
