Department of Radiology, Xiyuan Hospital, China Academy of Medical Sciences, Beijing, China.
Xiu-Xiang Liu
Email: liuxx2002@163.com
Received : Jun 23, 2025 Accepted : Aug 11, 2025 Published : Aug 18, 2025 Archived : www.meddiscoveries.org
Purpose: This study sought to explore the clinical characteristics and baseline MRI features of patients with anal fistulas, and to develop and validate a nomogram model using MRI data for predicting postoperative healing outcomes.
Materials and methods: We conducted a thorough evaluation to examine the association between clinical characteristics, baseline MRI findings, and postoperative healing in 307 patients with anal fistulas. Through logistic regression model, we identified key predictors of healing, which facilitated the creation and validation of a predictive nomogram model.
Results: The study comprised 307 patients, including 279 males (90.9%) and 28 females (9.1%), with ages ranging from 21 to 77 years (mean age: 40.13±12.70 years). Postoperatively, 280 patients (91.2%) achieved healing, while 27 (8.8%) did not. Logistic regression model identified several significant predictors of healing: prior anal fistula surgery, the number of external openings (≥2), fistula location, and fistula shape (all P<0.05). Using these factors, we developed a nomogram model to predict the likelihood of healing, with higher scores indicating a greater probability of successful outcomes.
Conclusions: The nomogram developed in this study, incorporating key clinical and MRI factors, exhibits robust predictive accuracy for postoperative healing of anal fistulas. With an AUC of 0.848 (95% CI: 0.757-0.938), this model shows significant potential in guiding clinical decision-making and improving the prognostic outcomes of anal fistula surgery.
Keywords: Anal fistulas; Magnetic resonance imaging; Nomogram; Prediction; Fistula healing.
The management and prognosis of anal fistulas remain significant clinical challenge, with surgery being the cornerstone of treatment. Successful surgical intervention necessitates a comprehensive understanding of the fistula’s pathological anatomy, particularly its relationship with the anal sphincter complex. The primary objective of surgery is to completely excise the fistula and any associated internal lesions while preserving anal sphincter function [1]. Although the Parks classification provides valuable insight into the fistula-sphincter relationship, it fails to address critical factors such as the fistula’s depth—defined as the distance from the highest point of the fistula to the anal verge on oblique coronal MRI-T2 weighted images—and its trajectory. These factors, which are not captured by the Parks classification, can significantly influence treatment outcomes.
Recent research have highlighted several prognostic factors that impact the success of anal fistula surgery. These include high transsphincteric fistulas, horseshoe fistulas, secondary tracts, anterior fistulas in females, and a history of previous fistula interventions [2-5]. While the anatomical depth and trajectory of the fistula are critical for developing a preoperative surgical strategy, limited research exists on their prognostic value in predicting postoperative outcomes. In the context of personalized medicine, predictive models are increasingly essential for guiding clinical decisions and improving patient outcomes. The nomogram, a graphical tool that integrates multiple clinical and radiological risk factors, has shown promise in predicting disease progression and treatment outcomes. It has been particularly effective in predicting tumor prognosis [6] and short-term postoperative outcomes in complex anal fistulas [7].
Magnetic Resonance Imaging (MRI) has proven highly accurate in delineating the anatomy of perianal fistulas, including the identification of internal openings and their intricate spatial relationships with the sphincter complex [8,9]. This accuracy is further enhanced by advanced imaging techniques such as T1- and T2-weighted imaging, Dynamic Contrast-Enhanced (DCE) imaging, and Diffusion-Weighted Imaging (DWI). These modalities facilitate both the qualitative differentiation between active and fibrotic fistula tracks and the quantitative assessment of fistula activity. In particular, DCE and DWI are pivotal in evaluating postoperative healing [7,10]. Moreover, MRI’s capacity to precisely visualize fistula depth, trajectory, and its pathological interactions with the sphincter complex provides essential information for strategic surgical planning. Beyond preoperative diagnosis, MRI plays a crucial role in postoperative monitoring, underscoring its vital contribution to anorectal surgery.
This study aims to develop a nomogram model, informed by MRI features, to enhance the assessment of patients’ responses to treatment and their risk of postoperative recurrence. By integrating detailed analyses of fistula depth, location, and trajectory, the model aspires to offer personalized and precise treatment strategies, thereby improving clinical outcomes for individuals undergoing anal fistula surgery.
Study population
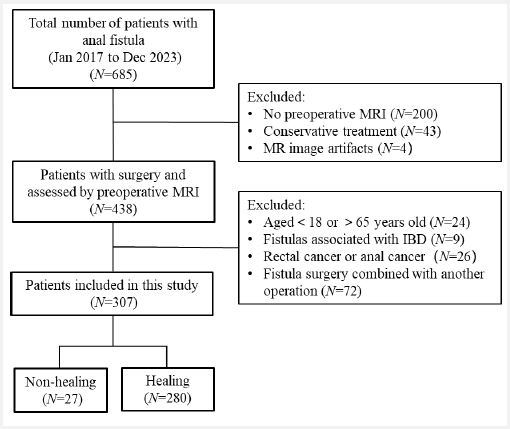
The dataset for this study was obtained from the Anorectal Surgery Center at Xiyuan Hospital, affiliated with the China Academy of Chinese Medical Sciences. Between January 2017 and December 2023, a cohort of 685 consecutive anal fistula patients was identified from our clinical database (Figure 1). Of these, 200 patients did not undergo preoperative MRI scanning, and 43 opted for preservation treatment. Additionally, MRI images from 4 patients were excluded due to artifacts. After applying the exclusion criteria, the study ultimately included 307 patients, consisting of 280 males and 27 females. Exclusion criteria were as follows: patients younger than 18 or older than 65 years, those with fistulas associated with Inflammatory Bowel Disease (IBD) or rectal or anal cancer, and cases where fistula surgery was performed in conjunction with another surgical procedure.
Clinical data collection
All patients underwent preoperative MRI to assess the anatomy of their anal fistulas. The patients included in this study were all diagnosed with anal fistulas, encompassing both low and high anal fistulas, as well as complex and simple types, and all underwent surgical treatment. Patients with complex high-level anal fistulas were managed using a staged surgical approach. The first stage involved the modified Henley operation, which focuses on resecting the branches outside the External Anal Sphincter (EAS) and placing loose setons around the sphincter. After 4 to 6 weeks, once the external opening has healed or is nearly healed, a delayed second-stage surgery is performed, consisting of seton removal and fistulotomy. In some cases, the seton will tighten and fall off spontaneously. Anal fistula surgeries at our center primarily include fistulectomy, fistulotomy, and seton surgery, with the seton serving both a drainage and chronic cutting function. We classify seton surgery as a form of fistulotomy. In total, 199 cases of anal fistulectomy and 108 cases of anal fistulotomy were performed. Clinical healing was defined as the absence of discharge from the external opening, which must be healed or nearly healed, with no clinical signs of perianal redness, swelling, heat, or pain, at 12 weeks post-surgery [11]. If the external opening remains unhealed with ongoing discharge, or if the external opening has healed but the patient still experiences discomfort around the anus that affects daily life, we define this as non-healing. In such cases, a delayed second-stage procedure, consisting of seton removal and fistulotomy, is required.
The study collected demographic data, including age, sex, alcohol consumption history, smoking status, prior anal surgery, and the presence of diabetes, hypertension, and hyperlipidemia. Alcohol consumption was classified based on current or previous habitual intake, defined as consuming alcohol one to two times per week, regardless of type or amount, and categorized into two groups: consumers and non-consumers [12,13]. Smoking status was determined based on self-reported cigarette use, defined as smoking five or more cigarettes daily for more than six months [14].
The anorectal surgeon will determine the number of external openings through digital anal examination. Additionally, during surgery, the distance from the external opening to the anal verge will be precisely measured.
The method of locating the internal opening on MRI
The location and number of internal openings were determined using the early arterial phase images (46.5s to 77.5s) from Dynamic Contrast-Enhanced (DCE) MRI, specifically in oblique transverse and coronal images. An internal opening is classified as “deep” if located beneath the external sphincter and “superficial” if above the external sphincter, as illustrated in Figure 2A.
Fistula depth measurement method
Fistula depth was quantified on oblique coronal T2-weighted MRI (T2WI) images by measuring the straight-line distance from the highest point of the fistula to the anal verge, as depicted in Figure 2B. The anal margin is identified on the oblique coronal T2WI as the lowest point of the subcutaneous portion of the external anal sphincter.
Fistula location
According to the Parks classification, a fistula is categorized as “high” if it is located above the deep portion of the external sphincter and as “low” if it is situated beneath the superficial portion of the external sphincter.
Fistula shape
Fistula paths are classified into two distinct categories. The first category is characterized by a linear trajectory, referred to as “ipsilateral” or “straight,” where the internal opening, fistula tract, and external opening are aligned on one side of the anal canal, suggesting either a transsphincteric or intersphincteric type. This type may range from the 12 o’clock to 6 o’clock positions or vice versa. The second category, in contrast, is curved, termed “contralateral” or “no fistula,” with the fistula extending from one side of the anal canal to the other, indicating a crossing—such as from the 12 o’clock to 6 o’clock positions or vice versa, as illustrated in Figure 2C.
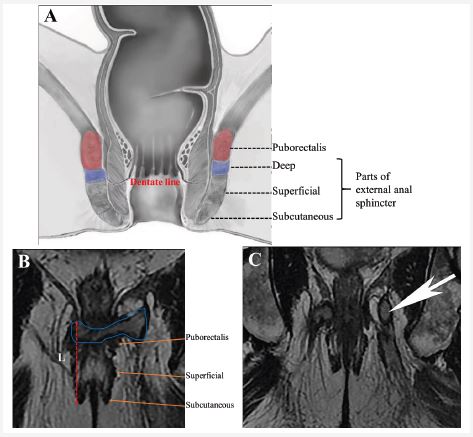
Image acquisition
Magnetic Resonance Imaging (MRI) examinations were conducted using a 3 Tesla MRI scanner (GE Medical Systems, Discovery-MR750) equipped with an 8-channel abdominal coil. No bowel preparation or anal canal intubation was undertaken prior to the scans. Patients were positioned supine for the MRI, with the positioning line aligned with the upper edge of the pubic symphysis. The protocol included a routine pelvic MRI focusing on the anal canal. Initially, sagittal plane images were acquired, followed by oblique axial scans perpendicular to the anal canal’s long axis, and concluding with oblique coronal scans parallel to this axis. Dynamic contrast-enhanced MRI examinations were performed on all patients, encompassing seven sequences— one prior to and six subsequent to contrast agent injection, with each sequence having a temporal resolution of 31 seconds. Gadoteridol was administered intravenously at a concentration of 0.1 mmol/kg (equivalent to 0.2 ml/kg of body weight) using an 18-gauge intravenous catheter connected to an automated injection pump (Optistar Elite, Mallinckrodt, Hazelwood, MO). Following the injection of the contrast medium, a 15 ml saline solution bolus was administered at a rate of 2 ml/sec. The parameters for the dynamic contrast-enhanced MRI included sequence type (T1-LAVA), acquisition plane (SPAIR axial), repetition time (4.5 msec), echo time (2.1 msec), flip angle (90 degrees), bandwidth (142.9 Hz/pixel), slice thickness with a gap (4.0 mm/2.0 mm), number of slices (616), acquisition matrix (256×224), field of view (260×234 mm), and an acquisition time of 3 minutes and 30 seconds. The scan time for the Diffusion-Weighted Imaging (DWI) MRI was 87 seconds.
Statistical analysis
Continuous data are summarized as medians and ranges, while categorical variables are reported as counts and percentages (%). Comparisons of continuous data were performed using the t-test, and categorical variables were analyzed using the Chi-square test or Fisher’s exact test, as appropriate. Univariate analysis was used to identify risk factors for fistula healing, with significant variables (P<0.05) subsequently included in a multivariate logistic regression analysis. The multivariate analysis identified prognostically significant factors, which were then used to develop a fistula-healing predictive model. This model was visualized as a nomogram, with its predictive accuracy evaluated using decision curve analysis and calibration curves. Statistical analyses were conducted with R software (version 4.1.0) and SPSS 25, considering P values<0.05 as statistically significant.
Relationship between clinical characteristics, baseline MRI characteristics and prognosis of anal fistula surgery
The baseline clinical characteristics of the 307 patients are summarized in Table 1, highlighting key demographic and health information. The cohort was predominantly male (279 males, 90.9%) compared to female (28 females, 9.1%). Of the 307 patients, 280 (91.2%) achieved clinical healing post-surgery, while 27 (8.8%) did not. A comparative analysis between the healed and non-healed groups, examining variables such as gender, age, smoking history, alcohol consumption, diabetes, hyperlipidemia, and hypertension, revealed no statistically significant differences (P>0.05). These findings suggest that these factors do not substantially influence the postoperative healing of anal fistulas.
A history of prior anal fistula surgery was significantly associated with healing outcomes. Specifically, 19.3% (54 cases) of patients with prior surgery achieved healing, whereas 51.9% (14 cases) did not, with a statistically significant difference observed (P=0.001). Additionally, the number of external openings, fistula location, and fistula depth were significantly associated with healing outcomes (P=0.02, P=0.0001, P=0.0001, respectively). Ipsilateral straight fistulas were more commonly observed in the healing group, while contralateral fistulas were predominantly found in the non-healing group. These results suggest that contralateral fistulas may be a significant factor influencing the postoperative healing of anal fistulas.
MRI findings were crucial in differentiating healing from non-healing outcomes. MRI results regarding the number of external openings, fistula location, and depth of the fistula showed significant differences between the healing and non-healing groups (P=0.02, P=0.02, P=0.0001, P=0.0001, respectively). This underscores the importance of MRI in assessing critical anatomical features that contribute to healing and non-healing outcomes.
| Patient characteristics | Healing | Non-healing | P |
|---|---|---|---|
| No. (%)/Median (range) | (N=280) | (N=27) | |
| Gender | 0.306 | ||
| Male | 253 | 26 | |
| Female | 27 | 1 | |
| Age (old; young-middle) | 0.289 | ||
| Old (≥60years) | 24 | 4 | |
| Young-middle (>18,<60 years) | 23 | 256 | |
| Smoking history (%) | 58 (20.7) | 2 (7.4) | 0.127 |
| Alcohol intake history (%) | 52 (18.6) | 4 (14.8) | 0.797 |
| Diabetes | 17 (6.1) | 1 (3.7) | 1 |
| Hyperlipidemia | 7 (2.5) | 0 (0) | 1 |
| Hypertension | 42 (15.0) | 1 (3.7) | 0.146 |
| Previous anal surgery(%) | 54 (19.3) | 14 (51.9) | 0.0001 |
| Second stage surgery | 76 (27.1) | 12 (4.3) | 0.058 |
| Surgical method | 0.526 | ||
| Incision | 97 | 11 | |
| Resection | 183 | 16 | |
| Number of external openings | 0.02 | ||
| 1 | 250 | 20 | |
| ≥2 | 30 | 7 | |
| Location of external opening | 0.482 | ||
| Front | 102 | 8 | |
| Back | 178 | 19 | |
| Number of fistulas | 0.071 | ||
| 1 | 193 | 14 | |
| ≥2 | 87 | 13 | |
| Fistula location | 0.0001 | ||
| Deep | 63 | 27 | |
| Superficial | 217 | 0 | |
| Number of internal openings | 0.541 | ||
| Uncertain | 12 | 0 | |
| 1 | 215 | 22 | |
| ≥2 | 53 | 5 | |
| Position of internal opening | 0.183 | ||
| Front | 109 | 7 | |
| Back | 171 | 109 | |
| Position of internal opening | 0.876 | ||
| Superficial | 79 | 8 | |
| Deep | 201 | 79 | |
| Depth of fistula (mm) | 0.0001 | ||
| <30 | 246 | 0 | |
| 30~45 | 25 | 6 | |
| >45 | 9 | 21 | |
| Location of fistula | 0.0001 | ||
| Superficial | 217 | 0 | |
| Deep | 63 | 27 | |
| Shape of fistula | 0.0001 | ||
| Contrealateral/no fistula | 71 | 22 | |
| Ipsilateral straight | 209 | 5 | |
| Parks classification | 0.451 | ||
| Intersphincteric | 135 | 12 | |
| Transsphincteric | 103 | 8 | |
| Subcutaneous | 3 | 0 | |
| Suprasphincteric | 2 | 0 | |
| Intermuscular abscess | 37 | 7 |
| Univariate regression | Multivariate regression | ||||||
|---|---|---|---|---|---|---|---|
| Characteristic | N | OR1 | 95% CI1 | p-value | OR1 | 95% CI1 | p-value |
| Age | 307 | ||||||
| Young-middle | — | — | |||||
| Old | 0.54 | 0.19, 1.95 | 0.3 | ||||
| Gender | 307 | ||||||
| Male | — | — | |||||
| Female | 2.77 | 0.55, 50.5 | 0.3 | ||||
| History of previoussurgery | 307 | ||||||
| Yes | — | — | — | — | |||
| No | 4.51 | 2.00, 10.3 | <0.001 | 4.87 | 1.92,12.9 | <0.001 | |
| Secondstage surgery | 307 | ||||||
| Yes | — | — | |||||
| No | 2.15 | 0.95, 4.79 | 0.062 | ||||
| Surgical method | 307 | ||||||
| Incision | — | — | |||||
| Resection | 1.30 | 0.56, 2.88 | 0.5 | ||||
| External opening | 307 | ||||||
| Front | — | — | |||||
| Back | 0.73 | 0.29, 1.68 | 0.5 | ||||
| Number of externalopenings | 307 | ||||||
| 1 | — | — | — | — | |||
| 1 | — | — | — | — | |||
| 1 | — | — | — | — | |||
| 1 | — | — | — | — | |||
| ≥2 | 0.34 | 0.14, 0.93 | 0.026 | 0.32 | 0.11,1.00 | 0.043 | |
| Number of fistulas | 307 | ||||||
| 1 | — | — | |||||
| 1 | — | — | |||||
| ≥2 | 0.49 | 0.22, 1.09 | 0.075 | ||||
| Fistula depth | 307 | ||||||
| <30 | — | — | |||||
| 30~45 | 0.00 | >0.9 | |||||
| >45 | 0.00 | 0.00,589,871,349,991,361, 868,522,884,808,266,626 |
>0.9 | ||||
| Fistula location | 307 | ||||||
| Deep | — | — | — | — | |||
| Superficial | 0.29 | 0.13, 0.66 | 0.003 | 3.13 | 1.04,9.73 | 0.043 | |
| Fistula shape | 307 | ||||||
| Univariate regression | Multivariate regression | ||||||
|---|---|---|---|---|---|---|---|
| Characteristic | N | OR1 | 95% CI1 | p-value | OR1 | 95% CI1 | p-value |
| Ipsilateral,straight | — | — | — | — | |||
| Contrealateral/no fistula | 0.08 | 0.03, 0.20 | <0.001 | 0.04 | 0.01,0.12 | <0.001 | |
| Internal_opening | 307 | ||||||
| None | — | — | |||||
| 1 | 0.00 | >0.9 | |||||
| ≥2 | 0.00 | 0.00,117,320,352, 807,511,801,866 |
>0.9 | ||||
| Postion_of_internal_opening | 305 | ||||||
| Front | — | — | |||||
| Back | 0.50 | 0.18, 1.21 | 0.15 | ||||
| Location_of_internal opening | 307 | ||||||
| Deep | — | — | |||||
| Superficial | 0.93 | 0.41, 2.34 | 0.9 | ||||
| Diabete | 307 | ||||||
| Yes | — | — | |||||
| No | 0.60 | 0.03, 3.09 | 0.6 | ||||
| Hyperlipidemia | 307 | ||||||
| Yes | — | — | |||||
| No | 0.00 | >0.9 | |||||
| Hypertension | 307 | ||||||
| Yes | — | — | |||||
| No | 0.22 | 0.01, 1.07 | 0.14 | ||||
| Smoking | 307 | ||||||
| Yes | — | — | |||||
| No | 0.31 | 0.05, 1.07 | 0.11 | ||||
| Drinking_alcohol | 307 | ||||||
| Yes | — | — | |||||
| No | 0.76 | 0.22, 2.09 | 0.6 | ||||
1OR: Odds Ratio; CI: Confidence Interval
Potential risk factors affecting surgical prognosis
The risk factors influencing the prognosis of anal fistula surgery are summarized in Table 2. The univariate analysis included variables such as sex, age, smoking history, alcohol consumption, diabetes, hyperlipidemia, hypertension, previous surgeries, the number and distance of external openings from the anal verge, the number and characteristics of fistulas (including their depth, location, and shape), the number and position of internal openings, and the surgical technique employed. The multivariate analysis revealed that factors such as a history of previous surgery (P=0.001), the number of external openings (N≥2) (P=0.043), fistula location (P=0.043), and fistula shape (P=0.001) may independently influence fistula healing, as shown in Table 2.
Nomogram construction
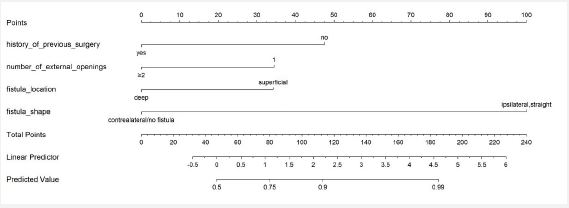
Based on insights from the multivariate analysis, four independent prognostic factors—history of anal surgery, number of external openings, fistula location, and fistula shape—were integrated to develop a predictive model for anal fistula healing, as depicted in Figure 3. The model is visualized through a nomogram, assuming a patient with no history of anal fistula surgery, one external opening (N=1), a superficial fistula location, and an ipsilateral straight fistula. Scores of 47.5 for no previous surgery, 98 for an ipsilateral straight fistula, 35 for one external opening (N=1), and 35 for a superficial fistula location, accumulating to a total of 184 points, suggest a 100% likelihood of healing.
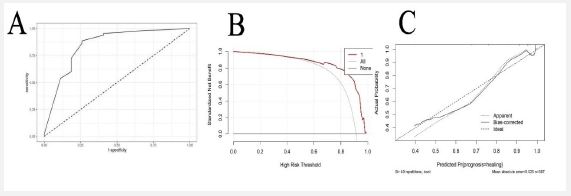
The model’s AUC value was 0.848, with a 95% Confidence Interval (CI) of 0.757-0.938, indicating its predictive accuracy. Moreover, the calibration curve confirmed the nomogram's potential utility in a clinical setting (Figure 4).
The management of anal fistulas presents a significant clinical challenge, particularly in selecting appropriate treatment strategies and identifying risk factors that influence postoperative healing. Recent research has increasingly focused on utilizing imaging characteristics to guide surgical planning and predict the risk of postoperative recurrence. The nomogram prediction model, validated for forecasting early postoperative healing outcomes of anal fistulas, integrates both clinical and MRI features to accurately predict surgical prognoses. This study identified surgical history, fistula shape, and the number of external openings as independent prognostic factors, aligning with the findings of Emile SH [15] and Raja MS [16]. A history of anal fistula surgery is a critical risk factor, as it may alter the tissue structure of the anal sphincter complex, complicating subsequent surgical interventions. Additionally, the morphology of the fistula and the presence of multiple external openings are indicative of disease complexity. Research has shown that an external opening located more than 2 cm from the anal verge is associated with increased lesion complexity [17] and a higher Parks classification, thus elevating surgical challenges and the likelihood of postoperative recurrence [16], as well as complications such as anal incontinence. Therefore, using a nomogram model based on MRI features enables a nuanced risk assessment, helping clinicians develop personalized treatment plans, select optimal surgical approaches, and ensure comprehensive postoperative care and follow-up.
Magnetic Resonance Imaging (MRI) plays a pivotal role in the preoperative assessment of anal fistulas, serving as the gold standard for their diagnosis. It provides anorectal surgeons with a detailed map of the surgical pathway, aiding in the evaluation of postoperative outcomes and potential complications. These insights not only enhance clinicians' understanding of anal fistulas but also assist in the strategic planning of surgical interventions. Specifically, the depth and morphological features of the fistulas are critical for developing appropriate surgical approaches.
In MRI-T2WI coronal images, a shallow fistula depth typically indicates that a direct resection approach is feasible. In contrast, deep and complex fistula paths, particularly those involving the puborectalis muscle, often require multi-stage surgical procedures. These cases demand not only the complete excision of lesions but also the preservation of sphincter function to avoid postoperative anal dysfunction and incontinence risks [18,19]. Therefore, for fistulas with significant depth, anal fistulotomy is recommended to alleviate symptoms and manage infection, thus preparing the patient for subsequent comprehensive treatment. Preoperative, precise measurement of fistula depth and evaluation of its morphological features are critical for assessing disease severity and formulating a personalized surgical strategy. This approach improves therapeutic outcomes, optimizes treatment efficacy, reduces symptoms, and lowers the risk of postoperative recurrence [20].
The nomogram, which combines key prognostic factors, offers a personalized tool for predicting anal fistula surgery outcomes. For patients with no prior fistula surgery, one external opening, a superficial fistula location, and an ipsilateral straight fistula, the model predicts a 100% likelihood of healing (score: 184 points). Its accuracy is supported by an AUC of 0.848 (95% CI: 0.757-0.938) and a calibration curve, demonstrating strong clinical utility. By integrating clinical and MRI data, the nomogram improves risk stratification and aids in planning individualized surgical strategies, especially for patients with complex fistulas at higher risk for recurrence and complications. This model enhances prognostic accuracy and treatment outcomes but requires larger, multicenter studies to confirm its generalizability and refine its application in diverse clinical settings [21].
Limitations of this study
This study has several inherent limitations due to its retrospective design and single-center setting. As a retrospective analysis, the reliance on existing patient records may introduce biases, such as incomplete data or inaccuracies in the recording of clinical and radiological findings. A more comprehensive evaluation of MRI parameters in predicting fistula healing could be achieved through a multicenter study, which would not only increase the diversity of the patient population but also improve the external validity of the results.
Additionally, the assessment of perianal abscesses was restricted to their size, without differentiating between specific types, such as horseshoe-shaped abscesses, or detailing their exact location within the anorectal space. Horseshoe-shaped abscesses, which are more complex in nature, may require different surgical approaches and have distinct prognostic implications. The lack of detailed classification may have limited the ability to fully assess their impact on healing outcomes.
Furthermore, the relatively small sample size in this study may have compromised the statistical power of some analyses. A larger cohort would improve the precision of estimates, enhance the accuracy of the predictive model, and allow for the detection of more subtle associations between variables. Given that our model was based on a single-center cohort, its applicability to other populations may be limited. Therefore, future multicenter, larger-scale studies are essential to validate and refine our findings, ensuring greater robustness and generalizability of the predictive model for anal fistula healing across diverse clinical settings.
Authors’ contributions: Xiuxiang Liu contributed to the research design, data collection, analysis, and paper revision. Hua Ren was involved in the research design, data collection, and analysis and took the lead in writing. Meng Wu provided support for this research and participated in the paper revision. Xiaochun Zhang provided support for the research and participated in the paper revision.
Funding: Construction of integrated platform for clinical scientific research of traditional Chinese medicine of Xiyuan Hospital of China Academy of Chinese Medical Sciences (Grant NO.XYZX0405-20).
Science and Technology Innovation Project of China Academy of Chinese Medical Sciences (Grant No. CI2021A03303).
Availability of data and materials: The data is uploaded to the submission system in Excel form.
Ethics approval and consent to participate: This retrospective study, conducted at a single institution, was approved by the Ethics Review Committee of Xiyuan Hospital, China Academy of Chinese Medical Sciences (2024XLA069-02). The requirement for written informed consent was waived by the Institutional Review Board. We confirm that all procedures were carried out in compliance with the relevant ethical guidelines and regulations.
Competing interests: The authors declare that they have no competing interests.
