1Resident, Department of Pathology, Armed Forces Medical College, India.
2Associate Professor, Department of Pathology, Armed Forces Medical College, India.
3Professor, Department of Pathology, Armed Forces Medical College, India.
4Professor and HOD, Armed Forces Medical college, India.
Gurpreet Kaur
Email: sagoo37@gmail.com
Received : Apr 12, 2025 Accepted : May 08, 2025 Published : May 15, 2025 Archived : www.meddiscoveries.org
Small Round Blue Cell Tumors (SRBCTs) include diverse group of aggressive pediatric malignancies that pose significant diagnostic challenges because of their overlapping histological features. These include Neuroblastoma (NB), rhabdomyosarcoma, non-Hodgkin’s lymphoma, Ewing’s sarcoma and the closely related Primitive Neuroectodermal Tumour (PNET) and the blastemic component of Wilms’ tumour. The tumours have similar appearance by light microscopy and are often indistinguishable by common immunocytochemical markers. Accurate diagnosis of this condition requires a comprehensive evaluation involving clinical presentation, imaging, histopathology, and immunohistochemistry. Herein, we report a rare case of a 3-year-old male presenting with right lower limb pain and a retroperitoneal mass with marrow involvement. This case highlights the diagnostic complexity of SRBCTs and the importance of a meticulous diagnostic approach in pediatric oncology. Timely diagnosis and intervention are crucial, guided by a high clinical suspicion and characteristic histopathological findings. Advances in treatment modalities offer hope for improved outcomes in this challenging malignancy.
Keywords: Small round blue cell; Neuroblastoma; Childhood malignancy.
SRBCTs covers a diverse group of undifferentiated or poorly differentiated malignancies that predominantly affect the children and adolescents. These tumors are characterized by small, round blue cells with scant cytoplasm and hyperchromatic nuclei. Accurate differentiation is very important, as each subtype has variable clinical symptoms, prognosis and treatment strategies.
The diagnostic challenge arises because of overlapping morphological features among these tumors. In many cases, patients may initially present with vague symptoms such as bone pain, fever, or fatigue. Imaging studies such as PET-CT (Positron Emission Tomography/ Computed Tomography) MRI and MIBG scans play an important role in identifying the extent of disease.
SRBCTs commonly infiltrate the bone marrow, where they may be mistaken for leukemia or lymphoma, further complicating the diagnosis. Bone marrow involvement is particularly common in high-risk tumors and it often signifies the advanced disease. Immunohistochemistry plays a very vital role in distinguishing between these malignancies and molecular studies are often required for confirmation. Most small round blue cells in BM pediatric pathology are attributable to leukaemias and lymphomas.
03-year-old male presented with pain right lower limb of one month duration associated with low grade fever. It was intermittent in nature, non-radiating, associated with limping gait, which aggravated on exertion and relieved on medication.
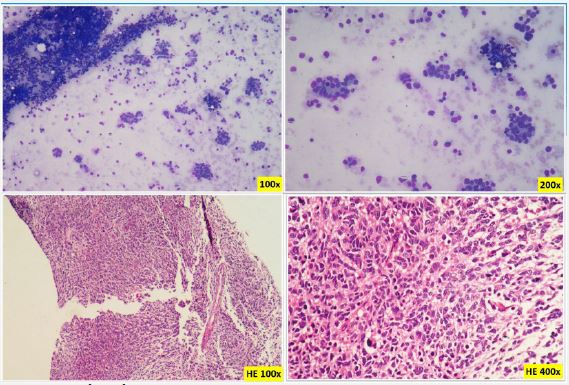
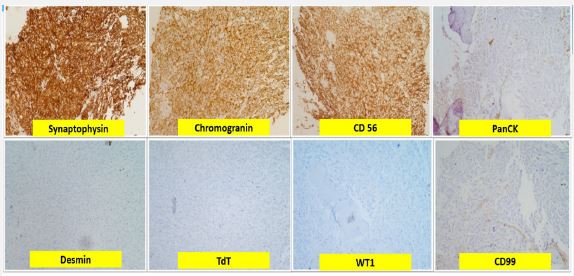
There was pallor, Hepatomegaly and tenderness over right hip joint. An initial diagnosis of ostemomyelitis was rendered and intravenous antibiotics were given. Ultra sonography abdomen revealed multiple paravertebral lesions in retro peritoneum and mediastinum and a mass lesion in right lobe of liver measuring 8.1×5.8×10 cm. The bone marrow aspirate revealed a cellular bone marrow aspirate showing small round blue cells forming rosettes places. These cells show high N:C ratio, scant cytoplasm, round to oval nuclei with stippled chromatin and inconspicuous nucleoli. Bone marrow biopsy showing normal marrow elements completely replaced by tumor cells in sheets as well as clusters forming rosette like morphology at places. These tumor cells had small round blue morphology with high N:C ratio, round to oval nuclei with salt and pepper chromatin and inconspicuous nucleoli and brisk mitosis (Figure 1) Immunohistochemistry (IHC) showed tumor cells that were positive for synaptophysin, chromogranin & CD56 and are negative for Pan CK, Desmin, Tdt, WT1 and CD99 (Figure 2). The combined histopathological and IHC findings were consistent with small round blue cell tumor. Cervical lymph node biopsy from the same patient also shows metastatic deposits of neuroblastoma, which was positive for chromogranin, CD99, CD56, Vimentin, ALK-1 with Ki67 proliferating index of 90% and negative for Pan CK, GFAP, SALL4, WT-1, p40, CD3, CD20, S-100.
| Differentials | Age | Common sites | Cytomorphology | IHC | Genetic features | Metastatic pattern |
|---|---|---|---|---|---|---|
| Neuroblastoma | Infants to young children | Adrenal gland,abdomen, chest | SRBCs, Homer Wrightrosettes | Synapto, Chromo,CD56 | MYCN amplification,ALK mutation | Bonemarrow, lymph nodes,lungs |
| Ewing Sarcoma | Children and adolescents | Bone, soft tissue | SRBCs in sheets | CD99, FLI1, NKX2.2 | EWSR1 translocation | Lung,Bone, Soft tissue |
| Rhabdomyosarcoma | Infants to adolescents | Headand Neck, GI tract | SRBCswith rhabdomyoblastic differentiation | Desmin, Myogenin, MyoD1 | FOXO1 translocation | Lungs, Lymphnodes, Bone |
| LymphoblasticLymphoma | Children and adolescents | Mediastinum,lymph nodes | Lymphoblasts with high N: C ratio, fine chromatin | TdT, CD3,CD79a | NOTCH1 mutations, TCRgene rearragements | Bone marrow,CNS, lymph nodes |
The diagnosis of SRBCTs is challenging due to their overlapping morphological features. Neuroblastoma, Ewing sarcoma, rhabdomyosarcoma, and lymphoblastic lymphoma are some of the common entities within this category, and distinguishing between them is very crucial for guiding appropriate treatment. In this case, the presence of rosette formation in the bone marrow aspirate, combined with positive immunohistochemical markers such as synaptophysin, chromogranin and CD56, favours a diagnosis of neuroblastoma.
Neuroblastoma commonly presents with Homer-Wright rosettes, but this feature can also appear in other SRBCTs. Ewing sarcoma, lacks rosette formation but it shows strong CD99 positivity and EWSR1 gene rearrangement, distinguishing it from neuroblastoma [2]. Rhabdomyosarcoma is another differential diagnosis which may mimic SRBCT morphology but it can also be confirmed by Desmin, Myogenin, and MyoD1 positivity [3]. Lymphoblastic lymphoma usually exhibits TdT positivity and lymphoid marker expression, which were negative in this case. Hence, immunohistochemistry plays an important role in excluding these entities and confirming the neuroendocrine profile of the tumor.
Imaging studies, particularly PET/CT and MIBG scans, provides very crucial insight into the extent of disease in this case. MIBG scanning is highly specific for neuroblastoma, while PET/CT helps in assessing metabolically active lesions across various malignancies [8]. Although the patient imaging strongly suggested neuroblastoma, histopathological confirmation was necessary to exclude the mimics. Molecular studies also play a very important role in refining the diagnosis [6]. Table 1 highlights important differential diagnosis to be considered in SRBCTS.
Accurate diagnosis of SRBCTs has therapeutic implications. In neuroblastoma, for risk stratification and treatment guidance, International Neuroblastoma Risk Group (INRG) classification system categorizes the patients based on their age, stage, MYCN amplification status, and histological differentiation [6]. While low-risk and intermediate-risk neuroblastoma may respond well to surgery or limited chemotherapy, high-risk disease often requires an intensive chemotherapy, surgical resection, radiotherapy, autologous stem cell transplantation and immunotherapy [4]. Immunotherapy also shows a promising improvement in survival rates for patients with high-risk or relapsed neuroblastoma. Anti-GD2 monoclonal antibodies and Chimeric Antigen Receptor (CAR) T-cell therapy are under investigation for their potential to enhance treatment efficacy recently [5]. In this case, confirming the diagnosis as neuroblastoma ensured that the patient was placed on an appropriate treatment regimen, avoiding unnecessary exposure to therapies intended for other malignancies.
This case illustrates the diagnostic dilemma in small round blue cell tumors in pediatric oncology. The overlapping morphological and immunophenotypic profiles demand a thorough, methodical approach for accurate diagnosis. Multimodal evaluation including imaging, histopathology, and immunohistochemistry is important to differentiate among entities such as neuroblastoma, Ewing sarcoma, and rhabdomyosarcoma and further guide the effective management strategies.
Advances in targeted therapy, immunotherapy and molecular profiling continue to improve the outcomes in patients with aggressive SRBCTs [5]. Ongoing research into novel therapies such as anti-GD2 monoclonal antibodies and CAR T-cell strategies offers hope for a better prognostic outcomes and long-term survival for children with small round blue cell tumors [9]. Additionally, molecular profiling is increasingly guiding personalized treatment strategies, improving survival outcomes by minimizing the treatment related toxicity. This case underscores the need for continued research and multidisciplinary collaboration to refine diagnostic strategies and expand treatment options for SRBCTs.
Author contributions: Data Curation: Dr Ankita Sharma; Writing: Dr Ankita Sharma, Gurpreet Kaur; Editing: Dr Ankur Ahuja.
Funding: This research received no external funding.
Informed consent statement: Informed consent was obtained from the subject.
