1School of Applied and Life Sciences, Uttaranchal University, India.
2Department of Biochemistry, All India Institute of Medical Sciences (AIIMS), India.
Alka Kumari
Email: alka.bchem@aiimsrishikesh.edu.in; alkakumari.aiims@gmail.com
Received : Apr 18, 2025 Accepted : May 05, 2025 Published : May 12, 2025 Archived : www.meddiscoveries.org
Gastroesophageal Reflux Disease (GERD) and Obstructive Sleep Apnea (OSA) are two prevalent medical conditions with significant global health implications. Emerging evidence suggests a bidirectional relationship between these disorders, with potential shared risk factors and pathophysiological mechanisms. This review examines the latest scientific understanding of the interrelationship between GERD and OSA, exploring underlying mechanisms, clinical implications, and recent advances in diagnostic and therapeutic technologies, including Artificial Intelligence (AI) and digital health tools. The review also discusses future research directions and the relevance of integrating multi-disciplinary approaches for optimal patient outcomes.
Gastroesophageal Reflux Disease (GERD) is a chronic condition characterized by the retrograde flow of gastric contents into the esophagus, leading to symptoms such as heartburn and regurgitation [21]. OSA, on the other hand, is a sleep disorder marked by repeated episodes of partial or complete upper airway obstruction during sleep, causing intermittent hypoxia and sleep fragmentation [16]. Both conditions are increasingly recognized for their comorbidities and potential to impact each other’s pathogenesis and progression. Recent advances in genetic epidemiology through Mendelian randomization analysis established stronger proof about the causal link between OSA and GERD [24].
The outcome of genetic research conducted during the period from 2023 until 2025 demonstrates a clear relationship between OSA and GERD development, so physicians now consider their mutual influence on each other’s progression [5]. At the same time technological progress revolutionizes the methods used for identification and treatment of these conditions. The use of digital health tools and Artificial Intelligence (AI) keeps increasing for better screening and diagnosis of OSA [1]. OSA risk detection through machine learning proves superior to routine screening processes because the algorithms use extensive datasets acquired from wearable devices alongside polysomnographic recordings [2]. These technologies enable medical staff to identify patients early and develop personalized treatment approaches which can adapt according to patient-specific GERD conditions together with individual symptom characteristics [20]. The main challenge in modern sleep and gastrointestinal medicine requires understanding of complicated GERD-OSA complex relationships. The clinical practice needs fundamental integration of genetic findings together with advanced digital tools and interdisciplinary team dynamics to achieve patient-centred total healthcare approaches [24]. The study examines the latest scientific evidence about GERD and OSA relationships along with the most recent breakthroughs and their clinical applications and emerging diagnostic tools and treatment modalities. The ongoing research is in favour of understanding disease connection pathways while promoting new patient care coordination studies to enhance treatment results.
GERD and OSA are prevalent worldwide, with estimates suggesting GERD affects approximately 20% of the adult population in Western countries [4], while OSA affects an estimated 9% to 38% of adults, depending on diagnostic criteria and population studied [17]. Studies indicate that up to 60% of OSA patients report GERD symptoms, highlighting a significant clinical overlap [8].
Two of the most prevalent chronic illnesses in general care and specialist settings are GERD and OSA. Concern concerning their overlapping clinical burden has grown as a result of their rising incidence globally, particularly in older and obese populations [10]. About 20% to 30% of people in the West suffer with GERD, and its prevalence is rising in Asia and the Middle East as a result of changes in food, lifestyle, and obesity rates [26]. On the other hand, OSA is thought to impact around 1 billion people worldwide, with moderate-to-severe forms affecting 9%-38% of the general population and more than 60% of obese or elderly people [12]. The statistical correlation between GERD and OSA exceeds random chance findings based on previous epidemiological data. Numerous research studies (2023-2025) reveal a wide co-occurrence ranging from 40% to 75% among patients who experience severe OSA or persistent GERD symptoms. The prevalence rate of dual GERD and OSA diagnosis remains higher than statistical chance rates especially among males but doctors now recognize that postmenopausal women run a specific risk of developing OSA [5].
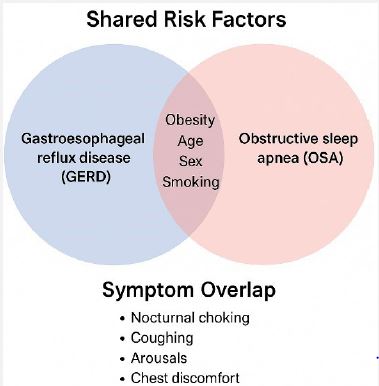
Numerous risk factors combine to explain the significant clinical connection between GERD and OSA while demonstrating their related pathophysiological patterns. Obesity functions as the main cause linking the two conditions because elevated BMI elevates intra-abdominal pressure while damaging diaphragmatic function and causing upper airway anatomic changes which result in worsened reflux as well as apneic events [18]. The recent fabrication of GLP-1 receptor agonist trials using tirzepatide and semaglutide has shown their capacity to enhance both weight reduction and decreases in Apnea-Hypopnea Index (AHI) metrics thus proving weight control’s essential role in treating OSA alongside GERD [11]. Smoking and drinking alcohol likely play a pathogenic role because they affect muscle tone by relaxing various oesophageal sphincters and pharyngeal dilators respectively in both GERD and OSA. The combination of sleeping on the back position with disrupted patterns of sleep increases the likelihood of harmful nocturnal reflux episodes as well as worsening of obstructive airway collapse [14]. The combination of common risk variables augments diagnosis odds while creating chances for combined screening efforts that focus on elimination of same causative mechanisms.
Numerous intricate and interconnected pathophysiological pathways support the link between GERD and OSA. Various processes shed light on possible areas for integrated treatment approaches and offer a framework for comprehending why various illnesses frequently co-occur.
The bidirectional relationship between GERD and OSA involves several hypothesized mechanisms:
Negative intrathoracic pressure: During apnoeic episodes, intrathoracic pressure decreases, promoting gastric content reflux. Negative intrathoracic pressure that builds up during obstructive apnoea’s represents a known mechanism that links OSA with GERD [18]. During sleep the upper airway collapse produces patients with OSA to generate intense inspiratory airway pressure before their airway clears. The great reduction of intrathoracic pressure generates an increase in transdiaphragmatic pressure gradient [15]. The gradient increase facilitates stomach contents to move back into the oesophagus especially when the Lower Eesophageal Sphincter (LES) tone is weak. The stomach reflux becomes much more pronounced when people sleep on their backs because this position decreases the gravitational resistance [13].
Arousal and transient LES relaxation: Sleep fragmentation in OSA may induce transient Lower Oesophageal Sphincter (LES) relaxation, facilitating reflux. OSA displays two hallmark features which include sleep arousals that arise because of hypoxemia together with increased breathing effort (X. Wang et al. 2023). Study data shows that TLES relaxations normally represent non-swallowing physiological events that lead to reflux both in healthy subjects and GERD patients when these arousals occur. The pathophysiology and persistence of GERD symptoms might be supported by the frequent arousals that occur in OSA thus leading to higher TLESRs [6]. A cyclic mechanism appears to exist where sleep disturbances first trigger reflux events yet night-time reflux identifies as a new cause of disrupted sleep patterns.
Inflammatory mediators: Chronic inflammation from reflux can affect upper airway reflexes, exacerbating OSA. In GERD, prolonged exposure to stomach acid can cause both local and systemic inflammatory reactions in the oesophagus and pharyngeal mucosa. The vagally mediated reflexes that control upper airway patency may be impacted by this inflammation, which can spread to the upper airway [22]. It has been demonstrated that acid-induced sensitization of the oesophageal- bronchial reflex arc increases airway reactivity and decreases pharyngeal dilator muscle tone, which may exacerbate airway collapse during sleep. Additionally, pro- inflammatory cytokines like TNF-α and IL-6, which are increased in both OSA and GERD, may exacerbate neuromuscular control of the upper airway and lead to systemic inflammation [9].
Obesity: A common risk factor that contributes to both GERD and OSA by increasing intra-abdominal pressure and fat deposition around the airway. In the pathophysiologic overlap between GERD and OSA, obesity is a known risk factor that may serve as a unifying etiological component (Shepherd and Orr 2016). By disrupting LES function and pushing stomach contents proximally, elevated intra-abdominal pressure brought on by central obesity encourages reflux [19]. Concurrently, fat accumulation in the neck and pharynx lowers airway diameter and raises collapsibility, two important aspects of OSA pathophysiology [3]. Furthermore, insulin resistance and systemic inflammation linked to obesity may exacerbate both illnesses by impairing neuromuscular function and gastrointestinal motility.
The accurate diagnosis of Obstructive Sleep Apnea (OSA) and Gastroesophageal Reflux Disease (GERD) depends on accurate diagnosis yet conventional diagnostic procedures currently work in isolation because clinical practice tends to isolate different diagnostic procedures. To diagnose GERD medical staff use three diagnostic methods which include upper gastrointestinal endoscopy combined with 24-hour esophageal pH or pH-impedance monitoring and GERD-Q symptom-based questionnaires. Therapeutic instruments check acid exposure alongside mucosal harm but they do not always detect either non-acidic or weakly acidic reflux which can occur elsewhere outside the oesophagus. The combination of several physiological measurements obtained through overnight PSG serves as the current standard to identify OSA by detecting breathing difficulties and sleep abnormalities and oxygen desaturation.
AI and ML technology revolutionized diagnostic methods within the last few years thereby enhancing both efficiency and precision and accessibility of OSA and GERD medical assessments. Analysis of PSG through AI algorithms establishes effective use in sleep medicine for automatic event assessment and sleep phase classification. The diagnostic reliability remains high but the processing duration and ratter disagreement rates sharply decrease through this method [23].
In GERD, AI-based methods are being developed to better analyze esophageal pH-impedance data. This would enable the diagnosis of episodes of non-acid reflux that may be missed by traditional pH monitoring. By identifying intricate impedance patterns and connecting them to the time of symptoms, these algorithms offer a more sophisticated comprehension of reflux load. The Structured State Space Sequence Model (S4) represents the most significant breakthrough by perfectly recognizing reflux events in 24-hour pH-impedance recordings. The diagnostic capability of this model demonstrates outstanding performance through an Area Under the Curve (AUC) of 0.87 and outmatches conventional software while matching expert assessment. The model identifies distant correlations within time series data collections. Zhou et al. [27] in Clinical and Translational Gastroenterology explain how machine learning systems advance impedance-pH monitoring diagnosis in GERD through improved clinical use and reduced observer variation and accelerated reflux event detection. The development and clinical application of AI technologies for reflux evaluation should proceeds alongside more accurate and personalization-based methods [27]. The accurate identification of disease conditions by practitioners and reduction of their workload depends on integrating deep learning systems into esophageal pH-impedance testing analysis. The identification of reflux episodes benefits from the deployment of ResNet-18 Convolutional Neural Network (CNN) as a deep learning model which executes image recognition activities. This CNN model received training for efficiently processing impedance-pH recordings by turning time-based physiological data into spatially arranged format. The ResNet-18 model achieved 84% diagnostic sensitivity together with an overall accuracy of 87% while identifying complex non- linear patterns associated with reflux episodes thus demonstrating its value for clinical application. This approach solves the limitations found in conventional methods and expert review since it proves efficient for detecting vulnerable data sources that exhibit artifact or non- acidic characteristics. High-throughput situations together with distant care benefits from the significant advancements made by CNNs to measure reflux load in GERD diagnosis through more efficient and repeatable and scalable methods [27].
The evolving understanding of the interrelationship between GERD and OSA highlights several key avenues for future research. Longitudinal prospective cohort studies need development because present evidence relies heavily on data from retrospective and cross- sectional approaches to link GERD with OSA. Establishing causality will serve both as a guiding factor for therapeutic approaches and it will help develop prevention strategies. The healthcare field needs comprehensive diagnostic tools which can detect GERD together with OSA when integrating diagnosis procedures. Given its potential to utilize wearable technologies alongside home-based sleep monitors and oesophageal pH-impedance testing the diagnostic platform improves efficiency and patient compliance through real-time multi-factor data collection. Scientific research must concentrate on several key domains because our knowledge about GERD-OSA connections continues to build. Longitudinal plus prospective cohort studies representing temporal and causal pathways must be developed for the understanding of these disorders because current research contains mostly retrospective and cross-sectional designs. Treatment selection and educational prevention strategies need clear evidence of causation to develop their strategies. Research requires the development of simultaneous diagnostic platforms that can assess OSA together with GERD during a single evaluation period. Electronic systems consisting of oesophageal pH-impedance testing in combination with wearable technology as well as home-based sleep monitors can enhance patient compliance through real-time multi-dimensional data collection for better diagnostic accuracy. These emerging directions underscore the importance of interdisciplinary collaboration among gastroenterologists, pulmonologists, sleep medicine specialists, and data scientists to generate holistic, patient-centered care models. Investment in these research priorities has the potential to not only improve clinical outcomes but also reduce the healthcare burden associated with these increasingly prevalent disorders.
