1Senior Lecturer, Igbinedion University, Okada, Nigeria.
2Icahn School of Medicine/Mount Sinai-Elmhurst Hospital, New York, USA.
Imesidayo Omua Eboreime-Oikeh
Tel: +234-810-933-2182;
Email: imesidayo.eboreime-oikeh@iuokada.edu.ng
Received : Apr 01, 2025 Accepted : May 02, 2025 Published : May 09, 2025 Archived : www.meddiscoveries.org
Chronic Kidney Disease of Unknown Etiology (CKDu) is an emerging epidemic disproportionately affecting agricultural workers in tropical and subtropical regions, with increasing reports from the late 20th to the 21st century. Unlike conventional Chronic Kidney Disease, CKDu is not associated with traditional risk factors such as diabetes, hypertension or glomerulonephritis, but is strongly linked to occupational and environmental exposures, particularly in Central America and South Asia. The geographical spread of CKDu is expanding, with recent reports from Africa and Europe. Chronic Kidney Disease of Unknown Etiology (CKDu) predominantly affects males in their third to fifth decades. Environmental drivers associated with CKDu include exposure to high ambient temperatures, agrochemicals, heavy metals, and contaminated water sources. This narrative review, conducted using a systematic search of large databases, explores recent advances in biomarker identification and epidemiological studies, examines environmental determinants, particularly the synergistic effects of heat stress and agrochemical exposure, and discusses challenges in early detection and the implementation of preventative measures in resource-limited settings. Limited resources and the complex nature of CKDu have hindered progress in establishing definitive etiological factors. Urgent international collaboration is required to establish effective diagnostic, treatment, and preventative strategies for this enigmatic disease.
Keywords: Agrochemicals; Chronic Kidney Disease of unknown etiology (CKDu); Environmental nephrotoxins; Heat stress; Heavy metals; Kidney disease epidemiology; Water contamination.
Chronic Kidney Disease of unknown etiology (CKDu) has emerged as a significant global health concern in the 21st century, particularly in Low-and Middle-Income Countries (LMICs), where it disproportionately affects young and middle-aged adults engaged in manual labor [1]. Unlike traditional Chronic Kidney Disease (CKD), CKDu occurs in individuals with no prior history of diabetes, hypertension, or other common risk factors. It has been notably reported in specific geographic hotspots, including Mesoamerica and South Asia, [2-4] where clusters of cases have been documented among agricultural workers exposed to high temperatures, recurrent dehydration, and potential environmental nephrotoxins.
CKDu is insidious, often presenting at advanced stages and progressing rapidly to end-stage renal disease, with an estimated annual mortality exceeding 30,000 [4]. In many affected regions, access to renal replacement therapy is limited or non-existent, resulting in high morbidity and mortality. Beyond the devastating health impact, CKDu places a severe burden on families and communities by affecting the working-age population and straining under-resourced health systems.
Despite increasing research interest, the etiology and pathogenesis of CKDu remain poorly understood. A wide range of potential risk factors has been proposed, including chronic heat stress, recurrent dehydration, exposure to agrochemicals and heavy metals, infectious agents, genetic predisposition, and socioeconomic determinants such as poverty, poor nutrition, and inadequate occupational protections [5]. However, the absence of a universally accepted case definition, coupled with methodological variability across studies, has hindered the development of consensus on causation, diagnosis, and management.
This review is motivated by the growing recognition that CKDu represents a distinct and pressing public health challenge. CKDu cuts across nephrology, occupational and environmental health, and global health equity. The rationale for this work lies in the fragmented nature of existing research and the urgent need for a more coherent synthesis of current knowledge. Numerous studies have explored the epidemiology and hypothesized risk factors of CKDu, but findings remain scattered across disciplines and settings, limiting their utility for guiding effective interventions.
A comprehensive review of recent advances in CKDu research is therefore both timely and necessary. This synthesis seeks to clarify the evolving epidemiological trends and burden of disease across different regions; consolidate emerging evidence on environmental, occupational, and social determinants; identify persistent knowledge gaps and methodological inconsistencies; and provide direction for future research, clinical management, and policy formulation.
By integrating current evidence and highlighting both progress and remaining challenges, this review aims to contribute meaningfully to the global discourse on CKDu. It offers an interdisciplinary perspective on the disease’s complex nature and outlines strategic priorities for addressing one of the most enigmatic kidney health threats of our time.
This narrative review employed a structured and systematic approach to identify, select, and synthesize relevant literature addressing Chronic Kidney Disease of Unknown Etiology (CKDu), with particular attention to environmental drivers, epidemiological patterns, and recent research advances.
Objectives
The objective of this review was to consolidate current evidence on CKDu in the 21st century, focusing on environmental risk factors (e.g., agrochemicals, heat stress, heavy metals, and water contamination), advances in disease understanding, and associated global health challenges.
Search strategy
We conducted a comprehensive literature search in the following electronic databases: PubMed, MEDLINE (via Ovid), Embase, and Global Health (via CABI)
The search included studies published between January 1, 2000, and March 31, 2025. We only considered studies published in English. The following key terms and Medical Subject Headings (MeSH) were used individually and in various Boolean combinations:
(“Chronic kidney disease of unknown etiology” OR CKDu OR “chronic kidney disease of nontraditional causes” OR “MesoMesoamerican nephropathy” OR CINAC OR “kidney disease of uncertain cause”) AND (“heat stress” OR “environmental nephrotoxins” OR “agrochemicals” OR pesticides OR herbicides OR “heavy metals” OR arsenic OR cadmium OR lead OR “water contamination” OR “groundwater quality” OR “climate exposure” OR “occupational risk factors”) AND (“epidemiology” OR prevalence OR incidence OR distribution OR risk factors OR “public health”) Search terms were adapted appropriately for each database’s-controlled vocabulary (e.g., Emtree in Embase).
Inclusion criteria
Articles addressing CKDu or CKD of unknown cause in human populations.
Studies examining associations between CKDu and environmental or occupational exposures.
Epidemiological surveys, cross-sectional and cohort studies, case series, and reviews.
Peer-reviewed articles published in English between 2000 and 2025.
Exclusion criteria
Studies focusing on CKD with established causes (e.g., diabetes, hypertension, glomerulonephritis).
Animal studies, in vitro experiments, or mechanistic studies not involving human populations.
Editorials, letters to the editor, opinion pieces, or publications without original data.
Study selection and data extraction
All identified titles and abstracts were screened for relevance. Full texts of potentially eligible studies were retrieved and reviewed for inclusion based on the predefined criteria. The data extraction process focused on the following variables:
Study location and population
Study design
Environmental or occupational exposure(s) assessed
Diagnostic criteria for CKDu
Key findings and conclusions
Reported limitations
We compiled the data in a structured spreadsheet to support narrative synthesis and thematic analysis.
Data synthesis and analysis
For this CKDu narrative review, we grouped our results thematically under the following headings and subheadings:
Epidemiological overview of CKDu
Regional CKDu hotspots
Environmental and occupational risk factors
Occupational heat stress and dehydration
Exposure to agrochemicals and heavy metals
Contaminated ground water and water hardness
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Low socioeconomic status and poor healthcare access
Genetic and epigenetic susceptibility
Multifactorial and region-specific etiologies
Recent advances
Understanding environmental factors
Improved epidemiological studies
Exploration of pathogenesis
Progress in potential interventions
Precision environmental health
Emerging biomarkers and early detection tools
Genetic testing
Public health interventions and policy responses
Current challenges
Research gaps
Future directions
Where appropriate, illustrative (Tables and Figures) were developed to summarize findings across studies.
Ethical approval was not required for this narrative review, as it did not involve human participants, animals, or identifiable personal data.
Epidemiological overview of CKDu
Chronic Kidney Disease of unknown etiology (CKDu) has emerged as a significant contributor to global kidney disease morbidity and mortality, particularly in tropical and subtropical regions. Unlike classical CKD, which is predominantly driven by diabetes mellitus and hypertension, CKDu typically affects young to middle-aged adults with no prior history of these risk factors. The global burden remains difficult to quantify precisely due to inconsistencies in case definitions, underdiagnosis, and limited surveillance, especially in low-resource settings [6,7]. Nevertheless, estimates suggest that tens of thousands of cases may occur annually in affected regions, with a substantial proportion progressing to End-Stage Renal Disease (ESRD).
Regional CKDu hotspots
Mesoamerica: CKDu has been documented extensively in regions where high ambient temperatures, intense labor, and agrochemical exposure are prevalent. The highest concentrations of CKDu cases have been reported from Central America, particularly among agricultural (sugarcane) workers in the Pacific coastal lowlands of Nicaragua and El Salvador. Termed Mesoamerican Nephropathy (MeN), the disease predominantly affects male sugarcane workers, many of whom develop renal impairment in their 30s or 40s. Cross-sectional studies have revealed CKDu prevalence rates ranging from 12% to 35% among high-risk occupational groups [8-10]. This regional epidemic has drawn significant international attention due to its scale and the young age of those affected.
South asia: In Sri Lanka and India, CKDu has emerged as a major public health problem, especially in rural paddy farming communities [7,11]. In the North Central Province (Anuradhapura and Polonnaruwa districts) of Sri Lanka, CKDu accounts for over 70% of all CKD cases in some areas [12,13]. Prevalence studies in affected regions have reported rates as high as 12% among adults [13]. Similarly, in Andhra Pradesh and Tamil Nadu in India, clusters of CKDu have been identified among rice and cotton farmers [14]. Despite regional variations, affected individuals often share similar occupational and environmental exposures.
Other emerging regions: CKDu-like presentations have also been reported in parts of Southeast Asia (e.g., Thailand), the Middle East, and among immigrant populations in the Gulf states [15-19]. While data from these areas are limited, demographic and occupational profiles were similar except in Thailand where CKDu prevalence was higher among females. Thai females play active roles in farming activities in Thailand. However, ongoing investigations have yet to unveil the factors contributing to the higher prevalence of CKDu in females. Further research is needed to fully understand the biological and social factors involved.
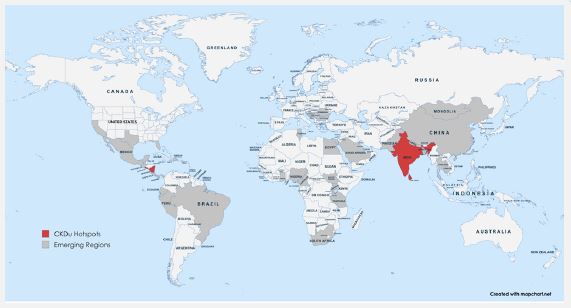
Growing evidence points to the presence of CKDu in parts of sub-Saharan Africa, although data remain sparse. A recent review of CKD in Uganda, Tanzania, Ghana, and Nigeria reported reduced kidney function in populations without traditional risk factors, suggesting a potentially significant but under-recognized burden of CKDu [20]. Reports of CKDu from other African countries are not uncommon [21]. Though national prevalence data are lacking; emerging evidence points to the presence of CKDu in rural agricultural populations in parts of Nigeria where the use of agrochemicals usually without adequate protective gear is nearly as high as 70% [22]. A recent cross-sectional study in Yobe State of Northern Nigeria reported a reduced Estimated Glomerular Filtration Rate (eGFR) in over 20.3% of adults with no history of diabetes or hypertension, suggesting possible CKDu [23]. Additionally, chronic exposure to agrochemicals and heavy metals, poor hydration during labor-intensive farming, and limited access to healthcare services may contribute to under-recognized CKDu cases in the country. Given the high prevalence of agricultural labor, extreme heat, and exposure to agrochemicals in many African countries, CKDu may be more widespread than currently appreciated (Figure 1). Shows the global distribution of CKDu.
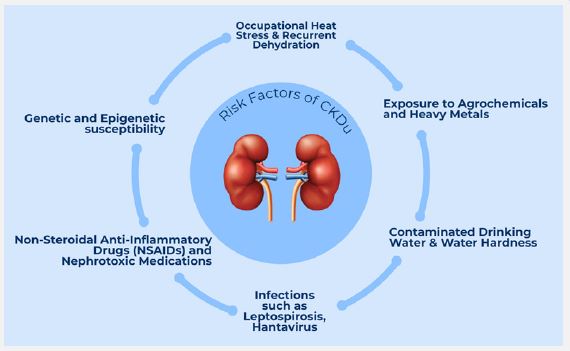
Despite its growing global footprint, the precise etiology of Chronic Kidney Disease of Unknown Origin (CKDu) remains elusive. However, a constellation of occupational, environmental, socioeconomic, and possibly genetic factors has been implicated. Despite regional variability in the interplay of these risk factors, several consistent themes have emerged across endemic settings, which are further elaborated below and visually represented in (Figure 2).
Occupational heat stress and dehydration
A widely accepted hypothesis suggests that recurrent dehydration and heat stress, aggravated by climate change and its associated global warming, are important contributors to CKDu pathogenesis [24]. Moreover, rehydrating with high fructose-containing drinks may exacerbate the nephrotoxic effect of heat stress and dehydration via a polyol-fructokinase mechanism [25]. Concurrent exposure to nephrotoxic agents, including Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), rhabdomyolysis from strenuous labor, illicit alcohol, agrochemicals, heavy metals, and environmental pollutants, may also aggravate renal damage associated with heat stress and dehydration [26]. Agricultural and manual laborers working in hot, humid conditions at low altitudes such as in the coastal regions of Mesoamerica, especially without access to adequate hydration and rest, are particularly vulnerable. Repeated episodes of subclinical kidney injury from volume depletion and heat strain may lead to progressive tubulointerstitial damage, ultimately resulting in heat-stress nephropathy. However, it has been postulated that heat stress may be a contributory, but not sufficient cause of CKDu. This is because chronic interstitial nephritis-associated CKDu is unusual in hotter Cuba and Myanmar where agrochemicals are sparingly used, along with the presence of CKDu among women, children and adolescents who are not exposed to the harsh working conditions [27].
Exposure to agrochemicals and heavy metals
Agrochemicals including pesticides, herbicides, and fertilizers are commonly employed in the agricultural regions with a high prevalence of CKDu. Studies from Sri Lanka and Central America have linked long-term agrochemical exposure especially glyphosate, paraquat, and organophosphates, with nephrotoxicity [27]. However, an analysis of groundwater in Chichigalpa, Nicaragua, where the highest prevalence of CKDu among men has been reported, did not detect elevated levels of any of the 57 pesticides tested. A key limitation of the study, however, was that only a single water sample was collected from each of the six study locations [28]. Nonetheless, concerns remain about the role of pesticides in the causation of Mesoamerican Nephropathy (MeN) [29]. Furthermore, toxic agrochemicals are considered among the leading potential contributors to CKDu in Sri Lanka [30]. Contamination of drinking water sources with heavy metals such as cadmium, arsenic, and lead has also been reported in some endemic areas, raising concerns about their potential role in renal damage of CKDu [31,32].
Contaminated ground water and water hardness
Water quality has emerged as a critical factor in CKDu pathogenesis. In Sri Lanka, for instance, high water hardness in endemic regions has raised concerns about the potential nephrotoxic effects of calcium and magnesium salts [33]. Additionally, the presence of fluoride, silica, and strontium in drinking water has been implicated as a contributing factor, warranting further investigation. It has been proposed that the interaction between water hardness and agrochemicals such as glyphosate may potentiate nephrotoxic effects [33].
Non-steroidal anti-inflammatory drugs
Chronic, unsupervised use of over-the-counter Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) to manage musculoskeletal pain from manual labor may also contribute to cumulative renal injury. These medications are known to impair renal perfusion, especially in dehydrated states, and may exacerbate subclinical kidney damage [34].
Low socioeconomic status
Although CKDu is increasingly being reported across the world, including the United States, [35] the populations most affected often reside in under-resourced settings with limited access to healthcare, delayed diagnosis, and inadequate treatment options. Malnutrition, limited education, and lack of awareness about hydration and occupational safety may further increase risk. Additionally, CKDu tends to progress silently until advanced stages due to poor access to early diagnostic services in underserved areas.
Genetic and epigenetic susceptibility
Although environmental factors are currently considered the primary drivers of CKDu, emerging research indicates that genetic predispositions or epigenetic modifications may increase individual susceptibility to environment- and occupation-related renal injury. Genetic involvement in CKDu remains inconclusive. While no specific high-risk genetic pattern is identified in Mesoamerican Nephropathy (MeN), studies suggest genetic risk factors in other CKDu forms. Notably, a rare KCNA10 gene variant correlated with Sri Lankan CKDu, and CYP1A1 polymorphisms, plus xenobiotic metabolizing enzyme genes, linked to Uddanam nephropathy, indicating potential gene-environment interactions [36-38]. Research suggests that environmental nephrotoxins such as agrochemicals and heavy metals may induce epigenetic alterations, including DNA methylation, histone modifications, and microRNA changes, impairing toxin detoxification and contributing to CKDu progression [39].
Multifactorial and region-specific etiologies
It is increasingly recognized that CKDu likely arises from multifactorial origins rather than a single causative agent. Regionspecific factors such as altitude, soil composition, farming practices, and cultural habits may interact with shared exposures to create localized risk profiles.
Understanding of environmental factors
Researchers are increasingly investigating the role of combined environmental exposures, such as the synergistic effects of heat stress, agrochemicals, and heavy metals. Studies are improving the understanding of how these exposures interact with individual susceptibility.
Improved epidemiological studies
Plans are underway to standardize epidemiological studies across different regions to improve data comparability and identify consistent risk factors. Initiatives like the DEGREE study (Disadvantaged populations estimated glomerular filtration rate epidemiology study) are working to establish standardized protocols estimate the burden of CKDu globally [40]. Geographic Information Systems (GIS) is being used to map CKDu prevalence and identify environmental hotspots, aiding in targeted interventions.
Exploration of pathogenesis
Research is turning to focus on the mechanisms of tubulointerstitial injury, a hallmark of CKDu, and how environmental exposures contribute to this process [41]. In addition, the role of inflammatory pathways in CKDu pathogenesis, is being investigated. The NLR family pyrin domain containing 3 (NLRP3) inflammasome plays an important role in inducing renal inflammation and fibrosis. Small molecule inhibitors targeting the NLRP3 inflammasome are potential agents for the treatment of CKD [42].
Precision environmental health approach
The burden of disease in humans largely depends on environmental exposures. Although generic preventive strategies, designed to mitigate environmental exposures such as promoting safe water practices and minimizing agrochemical application, have been instituted in certain CKDu hotspot areas, their impact has been inconsistent [43,44]. This limited impact may be due to suboptimal enforcement, restricted widespread adoption, or indeed, inherent inter-individual variability in response. Precision environmental health is an emerging field that aims to improve health outcomes through a nuanced understanding of human-environment interactions [45].
Emerging biomarkers and early detection tools
Given the late diagnosis of most CKDu cases, attention has shifted toward identifying non-invasive, early biomarkers that could signal kidney injury before irreversible damage occurs. Several promising biomarkers are currently being investigated for their potential clinical utility in CKDu. (Table 1) provides a summary of promising biomarkers currently under evaluation.
| Biomarker | Description | Potential role |
|---|---|---|
| Neutrophil Gelatinase-Associated Lipocalin (NGAL) | Urinary markerof tubular injury | Early detection of acute andchronic tubulointerstitial nephritis |
| Kidney InjuryMolecule-1 (KIM-1) | Expressed in proximal tubular cells after injury | Sensitive markerof subclinical kidneydamage |
| Beta-2 Microglobulin | Marker of proximal tubulardysfunction | May indicate early-stage CKDu in high-risk populations |
| Cystatin C | Serum markerof GFR | Less influenced by muscle massthan creatinine |
| Urinary N-acetyl-beta-D-glucosaminidase (NAG) | Lysosomal enzymereleased during tubularinjury | Potential for screening occupational groups |
Neutrophil Gelatinase-associated Lipocalin (NGAL) is a 25-kDa secretory protein that belongs to the lipocalin family. It is produced in response to epithelial injury within the renal tubules. NGAL is one of the leading new markers of renal epithelial injury [46]. In contrast to creatinine, which evaluates kidney function, NGAL is rapidly released into blood and urine following renal injury, making it a promising marker for early CKDu detection. Like NGAL, KIM-1, Beta-2 Microglobulin, and Urinary N-Acetyl-beta-D-Glucosaminidase (NAG) are released in response to renal tubular injury. Cystatin C, however, serves as a renal function marker analogous to creatinine, but offers improved accuracy. The biomarkers are still in varying phases of validation, and their integration into low-resource settings remains a challenge. However, they offer promising tools for future screening and risk stratification, particularly when paired with geospatial and occupational exposure data.
Genetic testing
Whole-genome sequencing has identified genetic mutations in approximately 25% of patients with previously unknown causes of kidney disease, highlighting the potential of genetic studies in CKDu diagnosis [47]. Clinical genetics is a growing field in nephrology. Nephrologists who care for individuals with kidney diseases including CKDu need to be able to recognize phenotypes, utilize genomics for diagnosis, and optimize patient care.
Public health responses
Despite the unclear etiology of CKDu, several individual-level and population-level strategies have emerged, aimed at mitigating progression of established disease, preventing new cases, and addressing the broader social, occupational, and environmental determinants.
Clinical monitoring and early detection
Early-stage CKDu often progresses silently, making routine monitoring crucial. For early diagnosis and management, high-risk individuals in endemic and non-endemic areas of Sri Lanka are screened in community settings through tests for serum creatinine, Glomerular Filtration Rate (GFR) estimation, Urine Albumin-Creatinine Ratio (UACR) and Blood Pressure (BP) [48].
Lifestyle and supportive therapy
Patients diagnosed with early CKDu are advised to avoid nephrotoxins (e.g., NSAIDs, contrast agents), maintain hydration, and adopt renal-friendly diets low in salt and protein. Supportive therapy with antihypertensives (if indicated) and close fluid balance monitoring are essential, although pharmacological options remain limited due to the lack of targeted therapy [48].
Education and behavior change
Patient education on safe water use and avoidance of suspected environmental exposures (e.g., contaminated water, agrochemicals) is a vital component of individual management. Mobile health initiatives and community health workers play a growing role in reinforcing these messages.
Occupational health interventions
Evidence from sugarcane workers in Central America suggests that implementing scheduled rest, shade, and hydration programs significantly reduces acute kidney injury episodes [49]. These strategies should be mandated and sustainability ensured in high-risk work environments, with government and employer accountability.
Environmental remediation and regulation
Promulgation of regulations on agrochemical use, water quality monitoring, and safe waste disposal is highly desirable, but issues with enforcement and sustainability are likely to hinder the impact. Ensuring access to clean drinking water free of fluoride and heavy metals has been a central intervention in endemic communities in Sri Lanka [50]. Similar measures should be adopted in other affected regions where appropriate.
Community-based surveillance
Developing grassroots surveillance systems for early identification of CKDu cases and exposure hotspots enables proactive responses. Integration of local health workers and NGOs has proven effective in awareness creation and early referral in Taiwan [51].
Health system strengthening
Policy-level interventions should focus on equipping primary health centers with tools for CKDu screening, training local healthcare providers, and subsidizing nephrology consultations and renal replacement therapy when necessary.
Despite growing recognition of CKDu as a significant global health issue, multiple challenges hinder progress in understanding and addressing the disease.
Unclear etiology and multifactorial risks
The precise cause of CKDu remains unknown, with multiple hypotheses involving heat stress, dehydration, agrochemical exposure, heavy metals, infections, and genetic predisposition. However, no single factor has been definitively proven as the primary cause. It is possible that multiple factors, or their complex interplay, underlie the pathogenesis of CKDu, which is also referred to as chronic kidney disease of multifactorial origin (CKDmfo).
Due to its unclear etiology, this enigmatic disease has been described using a variety of terms, including Chronic Kidney Disease of Nontraditional Etiology (CKDnt), Chronic Interstitial Nephritis in Agricultural Communities (CINAC), Kidney Illness of Unknown Cause in Horticultural Workers, and Kidney Disease of Unknown Cause in Agricultural Laborers (KDUCAL) [52,53] Approximately a decade ago, some researchers proposed the term Nephropathy of Unknown Cause in Agricultural Labourers (NUCAL) as a replacement for Mesoamerican Nephropathy (MeN); however, the proposed nomenclature did not gain widespread acceptance [54,55]. The variety of terms applied to CKDu highlights the ongoing debate within the scientific community and the critical need for a unified global definition, along with a comprehensive understanding of its etiology.
Lack of a standardized case definition
Different regions use varying diagnostic criteria for CKDu, complicating comparisons across studies [56,57]. The absence of universally accepted biomarkers for early detection further limits diagnosis and intervention efforts.
Limited longitudinal and mechanistic studies
Most existing studies are cross-sectional, making it difficult to establish causal relationships [58]. There is a need for prospective cohort studies and mechanistic research to understand disease progression.
Health system constraints in affected regions
CKDu primarily affects agricultural workers in LMICs, where healthcare access is limited, renal replacement therapy is unavailable, and disease surveillance is weak. Many affected individuals lack access to early diagnosis and supportive care.
Socioeconomic and occupational barriers
CKDu disproportionately affects low-income, marginalized communities with hazardous working conditions. Effective CKDu mitigation necessitates policy interventions that enhance labor protections, ensure access to hydration, and implement robust environmental safety measures, thereby addressing health inequities.
Insufficient global policy response
Unlike other renal pathologies, CKDu has not elicited a coordinated global response from international health organizations [6]. Rectifying this deficiency is essential to facilitate future research and policy endeavors aimed at enhancing early detection, refining disease classification, and implementing efficacious prevention strategies within affected populations. Research funding and public health initiatives remain inadequate compared to the growing burden of the disease.
By addressing these challenges, future research and policy efforts can move toward improving early detection, refining disease classification, and implementing effective prevention strategies in affected populations.
Key research gaps and future directions
Despite increasing recognition of CKDu as a public health threat, significant gaps persist in understanding its etiology, diagnosis, prevention, and management. Addressing these knowledge deficits is critical for developing targeted and context-specific interventions.
Lack of consensus on case definition
One of the fundamental barriers to CKDu research is the absence of a universally accepted case definition. Current diagnostic criteria vary across studies and countries, hindering data comparability and pooled analyses. Future studies should aim to validate standardized diagnostic criteria tailored to endemic settings and stratify cases based on severity, etiology, and progression.
Limited longitudinal and mechanistic studies
Most available studies are cross-sectional, limiting causal inferences. There is a pressing need for prospective cohort studies and experimental models to elucidate temporal relationships and biological mechanisms linking environmental and occupational exposures to kidney injury.
Inadequate data from underrepresented regions
While CKDu has been extensively documented in Central America, South Asia, and parts of Southeast Asia, there is limited epidemiological and clinical research from Sub-Saharan Africa. Region-specific studies are essential to determine whether similar patterns exist and to inform localized interventions.
Emerging role of climate change
Rising global temperatures may exacerbate occupational heat stress, especially in tropical and subtropical regions. Few studies have quantitatively examined the relationship between climate variables and CKDu incidence. Future research should model the impact of climate change on CKDu risk and incorporate climate resilience into prevention strategies.
Biomarker discovery and validation
Emerging urinary and serum biomarkers such as NGAL, KIM-1, and beta-2 microglobulin—show promise for early detection of tubular damage yet require validation in CKDu-endemic populations. Integration of omics approaches (proteomics, metabolomics, epigenomics) could also uncover novel pathways and diagnostic tools.
Gaps in policy and recommendations
Even where environmental and occupational guidelines exist, compliance and enforcement remain weak. Dissemination and Implementation (D&I) Science, a field focused on translating evidence-based interventions into real-world settings, can effectively identify barriers and facilitators to policy uptake, particularly in low-resource contexts.
Policy recommendations for mitigating CKDu
The growing prevalence of CKDu, particularly among low-income, rural, and agricultural communities, underscores the urgent need for evidence-informed policies. Mitigation strategies must go beyond individual behavior change to encompass structural and environmental reforms that address the root causes of CKDu.
| Policy area | Recommendation | Target stakeholders |
|---|---|---|
| Agrochemical regulation | Enforce labeling, safety training, and restricted use | Ministries of Agriculture, Environmental Protection Agencies |
| Occupational health | Mandate hydration, rest breaks, and protective gear | Labor Departments, Employers |
| Water quality | Monitor and purify watersources in endemicareas | Water Boards,Local Governments |
| Health systemintegration | Include CKDuin NCD strategies and training curricula | Ministries of Health, Primary Care Facilities |
| Research and surveillance | Increase fundingand promote regional studies | Academic institutions, International donors |
| Community involvement | Develop culturally adapted, community-led education | NGOs, Civil Society, Traditional Leaders |
Strengthen regulatory frameworks
Governments should enforce stricter regulations on the production, importation, distribution, and use of agrochemicals. Policies mandating proper labeling, protective equipment use, and safe storage can reduce occupational exposure. Monitoring and regulating heavy metal contamination in drinking water sources should also be prioritized.
Occupational safety standards
Implementing and enforcing labor protection policies for workers in high-temperature and physically demanding settings is vital. This includes the provision of shaded rest areas, access to clean drinking water, work-rest cycles, and education on the dangers of heat stress and dehydration.
Surveillance and infrastructure
Developing reliable water testing and purification infrastructure is essential in rural areas where water hardness and contamination are suspected CKDu contributors. Investing in climate-resilient public utilities and agricultural practices can also mitigate environmental risks.
Integrated health systems approach
Public health systems should incorporate CKDu into national Non-Communicable Disease (NCD) action plans. Early detection and surveillance programs, training of primary healthcare providers, and integration of CKDu management into routine care are necessary to strengthen health system preparedness.
Research funding and international partnerships
Dedicated funding for CKDu research, especially in underrepresented regions such as Sub-Saharan Africa, is critical to closing data gaps. International collaboration and knowledge exchange platforms can help disseminate best practices and promote regionally appropriate interventions.
Community engagement and policy co-design
Engaging communities in co-creating policies ensures local relevance and buy-in. Participatory approaches, such as citizen science, peer education, and inclusion of local leaders in health governance, can enhance the acceptability and sustainability of interventions.
The Policy Recommendations are summarized in (Table 2).
Chronic Kidney Disease of Unknown Origin (CKDu) represents an urgent and growing public health challenge, particularly in tropical and subtropical regions where agricultural workers are at increased risk due to environmental and occupational exposures. The pathogenesis of the disease is still poorly understood, with many questions yet to be answered regarding its exact causes. However, considerable strides have been made in identifying potential environmental and occupational risk factors, including exposure to agrochemicals, heavy metals, contaminated water, and heat stress.
This review has highlighted the expanding geographical reach of CKDu, with new reports emerging from regions previously unaffected by the disease, such as parts of Africa and the Middle East. These findings highlight the global nature of the CKDu crisis and the need for a unified, international approach to address it. Recent research has pointed to the cumulative effects of multiple environmental toxins, which may act synergistically to cause kidney injury in susceptible individuals. Moreover, genetic susceptibility plays a critical role in determining who is most at risk, suggesting that future research should explore this dimension more deeply.
The healthcare burden associated with CKDu is severe, with affected individuals often presenting at advanced stages of kidney disease. Early diagnosis, screening programs, and preventive measures must be prioritized, particularly in high-risk populations. Healthcare systems in affected regions are currently ill-equipped to manage the burden of CKDu, necessitating urgent reforms in healthcare infrastructure, public health education, and training of healthcare providers. Additionally, the lack of international collaboration in CKDu research and policymaking remains a major obstacle. The spread of the disease across borders calls for greater cooperation between governments, international organizations, and research institutions to share data, resources, and expertise. Global health organizations like the World Health Organization (WHO) must take a leading role in facilitating these efforts.
In conclusion, while progress has been made in understanding CKDu, much remains to be done. Continued research into the environmental drivers, molecular mechanisms, and genetic susceptibility of CKDu will be critical for developing targeted interventions. Furthermore, a more coordinated global response is necessary to mitigate the health, social, and economic impacts of this devastating disease. By addressing both the root causes and the healthcare challenges associated with CKDu, we can work toward minimizing its impact on affected communities and preventing further spread of the disease.
Conflict of interest: The authors declare that they do not have conflicts of interest.
Funding: The authors did not receive any funding for this work.
Author contributions
IOE-O conceptualized the review, designed the search strategy, and led the writing of the manuscript.
OSO contributed to literature screening, data extraction, and drafting of key sections.
Both authors methodology, reviewed the included studies, and contributed to the interpretation of findings, critically revised the manuscript for important intellectual content and assisted in final editing and formatting.
Both authors read and approved the final version of the manuscript and have no intention of benefitting financially from the submitted manuscript.
Acknowledgements: The authors express their gratitude to colleagues, health professionals, and researchers whose work and field experiences have contributed to the understanding of CKDu.
We extend our appreciation to Ms. Rebecca Josiah, a fifth-year medical student, for her assistance with the graphics.
