1Inner Mongolia Autonomous Region People’s Hospital, Hohhot 010010, China.
2Inner Mongolia Autonomous Region Hospital of Traditional Chinese Medicine, Hohhot 010010, China.
†These authors contributed equally to this paper.
An-Juan
Email: hsjbggwsbgs@163.com
Received : Oct 01, 2024 Accepted : Oct 22, 2024 Published : Oct 29, 2024 Archived : www.meddiscoveries.org
A 53-year-old man presented with abdominal distension and vomiting lasting three months. Further examination in the ward confirmed a diagnosis of antral malignant tumor with pyloric obstruction. The patient was then transferred to surgical oncology. After evaluation, laparoscopic large gastrectomy with gastrojejunostomy was performed under general anesthesia without absolute contraindications. Following the operation, the patient received enteral and external nutritional support, anti-inflammatory medications, acid suppression therapy, and anti-tumor treatments. The patient’s condition steadily improved.
On the 7th day post-surgery, the patient developed a low-grade fever but no other uncomfortable symptoms, and his condition improved after symptomatic treatment. On the 10th day post-surgery, the patient experienced malignant hyperthermia, with a maximum body temperature of 39.5°C. Routine blood tests indicated leukopenia (white blood cells at 0.64 × 109/L), anemia (red blood cells at 2.84 × 1012/L), and thrombocytopenia (platelets at 22 × 109/L). Immunoassay results showed procalcitonin (PCT) at 85.670 ng/ml. CT of the head and chest, abdominal ultrasound, and incision dressing change were performed to rule out lung and abdominal infections, as well as surgical incision infection. The ICU consultation considered potential sepsis and septic shock. It was recommended to initiate broad-spectrum antibiotic combination therapy, conduct blood cultures, and replace the deep venous catheter.
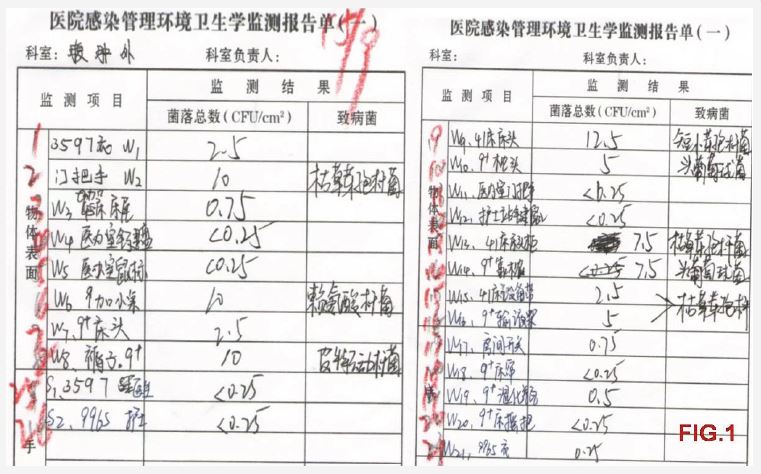
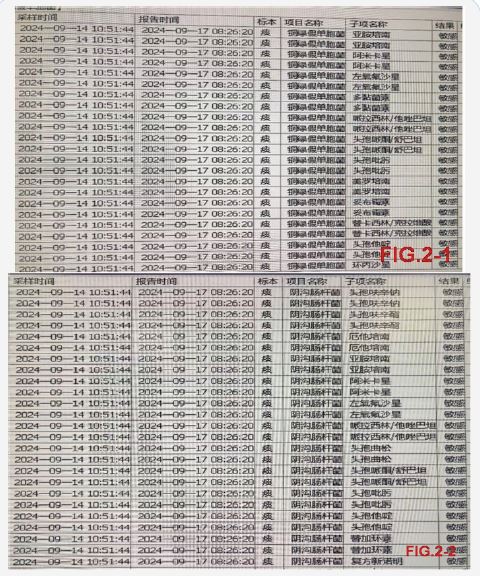
Sampling and monitoring of high-frequency exposure of patients (Figure 1) were conducted. The results of environmental sampling showed that Pseudomonas aeruginosa was not detected in the high-frequency environment of the patient, but various pathogenic bacteria such as Bacillus subtilis, Lysine bacillus, and Bacillus breve were detected. It was recommended to strengthen the daily cleaning and disinfection of the ward.The microbiological test report (Figure 2) indicated that Pseudomonas aeruginosa was detected in peripheral blood culture, with antimicrobial susceptibility results showing sensitivity and no drug resistance. Pseudomonas aeruginosa was also detected in deep vein blood culture, with sensitivity and no resistance. Sputum cultures detected Enterobacter cloacae and Pseudomonas aeruginosa, with susceptibility results indicating sensitivity and non-resistance. The patient continued to receive broad-spectrum antimicrobial therapy based on the results of drug susceptibility.
On the 13th day post-surgery, the patient was in a coma, with a sudden drop in blood pressure and impaired consciousness. Blood pressure was recorded at 60/33 mmHg, blood oxygen fluctuated around 80%, and the patient was breathing 30 times per minute. Norepinephrine (NE) was administered along with other related treatments, but the patient’s indicators did not improve. Invasive ventilator-assisted treatment was initiated; however, the patient’s family refused to carry out invasive treatment measures.
The patient’s vital signs did not improve on the same day and ECG monitoring and ventilator were stopped according to the wishes of the family, so all drugs were stopped, then the patient’s breathing, heartbeat stopped, the light reflex disappeared, the ECG showed total cardiac arrest, and the cardiac activity disappeared, and the patient was declared clinically dead.
Septic shock is often complicated by surgery, severe burns, trauma, and infections. It is an acute and progressive condition with a high mortality rate [1]. Despite advanced diagnostic and treatment measures, septic shock remains a leading cause of death among critically ill patients. Our studies indicate that the case fatality rate for septic shock is approximately 35% [2]. The primary cause of septic shock is infection from various pathogens
In this case, Pseudomonas aeruginosa was identified in the sputum culture, peripheral blood culture, and deep vein blood culture of the patient with septic shock. Previous studies have shown [4] that gram-negative bacteria dominate the culture of pathogenic bacteria in septic shock patients, with Acinetobacter baumannii and Pseudomonas aeruginosa being the most significant pathogens. This aligns with our findings.
These two types of bacteria are common conditionally pathogenic organisms that cause nosocomial infections. The widespread use of broad-spectrum antibiotics, immunosuppressants, and invasive monitoring techniques has led to an increase in nosocomial infections. This highlights the urgent need to implement multimodal infection control strategies. The World Health Organization (WHO) proposed in the 2016 Core Content of the National and Acute Care Facility Hospital Infection Prevention and Control Project that a multimodal intervention strategy is the most effective way to successfully implement infection control [5].
Although Pseudomonas aeruginosa and Enterobacter cloacae were not detected, various pathogenic bacteria such as Bacillus subtilis, Lysine bacillus, and Bacillus breve were found in the high-frequency environment of the ward, indicating that daily cleaning and disinfection practices were inadequate. Additionally, it is essential to strengthen the management and training of hand hygiene. The WHO reported in the Guidelines on Hand Hygiene in Healthcare Facilities, updated in 2009, that hand hygiene is one of the simplest and most effective measures for the prevention and control of nosocomial infections [6].
In summary, postoperative patients are prone to septic shock, with respiratory tract infections being the primary infection site. The distribution of pathogenic bacteria is predominantly gram-negative, such as Pseudomonas aeruginosa. This retrospective analysis of septic shock mortality cases provides a reference for future targeted measures to prevent infection.
