Ragus Healthcare Pvt Ltd, Sugar. Fit, HSR Layout, Sector 3, Bengaluru, Karnataka 560102, India.
Annie Mattilda Raymond
Email: annie.mattilda@sugarfit.com
Received : Aug 10, 2024 Accepted : Sep 23, 2024 Published : Sep 30, 2024 Archived : www.meddiscoveries.org
Type 2 diabetes is described as a combination of low amounts of insulin production from pancreatic β-cells and peripheral insulin resistance [1]. One of insulin’s primary functions is its role as an anabolic hormone. It significantly enhances glycogen synthesis in the liver and muscles, promoting the storage of glucose as glycogen. Furthermore, insulin stimulates protein synthesis and inhibits proteolysis. By enhancing glycogen and protein synthesis, insulin supports the maintenance and growth of muscle tissue and plays a crucial role in regulating overall energy metabolism and maintaining glucose homeostasis. Insulin resistance is a critical factor in the disease process, as well as in fat storage and mobilization [2]. As populations age, the prevalence of type 2 diabetes increases because insulin resistance tends to increase with age. The prevalence of diabetes has surged in developed and developing countries during the last four decades. This rise can be attributed to the abundance of food, subsequent shifts in dietary patterns, and a decrease in physical activity levels [3]. Individuals who are overweight or obese typically experience some degree of insulin resistance, yet diabetes only manifests in those who do not produce enough insulin to counteract this resistance. Despite potentially high levels of insulin in these individuals, it remains insufficient to normalise glycemia levels leading to poor glycaemic control [4]. This poor glycaemic control is a key risk factor for albuminuria. Recent studies using HbA1C have shown a correlation between poor glycemic control and albuminuria, while intensive glucose control reduces this risk [5]. Albuminuria is a well-known predictor of poor renal outcomes in patients with type 2 diabetes, and can be characterised by the abnormal loss of albumin in the urine, followed by a decline in Glomerular Filtration Rate (GFR), which leads to end-stage renal disease. Screening for elevated urine albumin is of greatest clinical importance for preventing or alleviating diabetic kidney disease at its early stage [6]. Patients with albuminuria exhibit widespread vascular damage [7] due to a systemic endothelial disorder also affecting the glomerular endothelium. This endothelial disorder has been linked to an elevated glomerular and vascular oxidative stress in patients with albuminuria [9]. This endothelial dysfunction is a common feature of diabetes and closely related to insulin resistance [10]. Clinically, the presence of albuminuria is associated with a high risk of renal functional loss over time. This association is found in various diseases such as diabetes mellitus, and hypertensive kidney disease [11]. In addition to albuminuria, the biomarkers such as serum urea and creatinine are known to be raised in cases of hyperglycaemia in uncontrolled diabetics, which indicates severity of kidney damage [12]. The renal function is assessed by measuring urinary albumin-to-creatinine ratio in patients with Type 2 Diabetes (T2D) [13]. Recent studies show that nutritional education and dietary counselling are essential within primary, secondary, and tertiary T2DM clinical care settings aiding individuals understand their food and beverage consumption behaviours and develop the skills needed to manage their diabetes effectively and prevent related comorbidities [14]. These approaches focus on measuring HbA1c as a key T2DM outcome, while secondary outcomes are only addressed through persuasive weight management and behavioural lifestyle changes [15]. Therefore, caloric restriction-based personalized lifestyle recommendations are also crucial for an effective T2DM prevention strategy. Furthermore, behavioural interventions for managing both diabetes and hypertension emphasise the importance of comprehensive lifestyle modifications, including diet, exercise, weight management, strength training, cardio exercises and medication adherence. The integration of these lifestyle modifications allows the individuals to achieve better glycaemic control, manage hypertension more effectively, and enhance their overall health outcomes. The case study highlights the success of a comprehensive program, Sugarfit’s Diabetes Reversal and Management Program (SDRMP), in reversing diabetes by achieving significant improvements in blood sugar levels and improving overall health outcomes. It seems to focus on a holistic approach to diabetes management by consistently integrating personalized coaching aimed at improving diet, exercise, and overall lifestyle habits with medications. This approach acknowledges the importance of lifestyle modifications along with medication at reduced dosage and frequency, which leads to more sustainable and long-term management of diabetes by regulating blood sugar levels more effectively, reducing albuminuria, enhancing muscle strength, promoting a healthier lifestyle, and improving the quality of life for individuals with diabetes. Additionally, the inclusion of empathetic coaching suggests a focus on emotional support and motivation, which can be crucial in sustaining long-term lifestyle changes. Overall, this approach reflects a comprehensive understanding of diabetes management, addressing not only the physiological aspects of the condition but also the behavioural and emotional factors that influence it. This aimed to evince the success of a complete program in achieving long-lasting recovery, a significant shift in levels of glycated Haemoglobin (HbA1c), average blood glucose, weight, Fasting Blood Sugar (FBS), and Body Mass Index (BMI), and notable enhancements in overall health.
This presents the case of Mr. CP, a 42-year-old male with type 2 diabetes and essential hypertension. He enrolled in the Sugarfits diabetes reversal and management program in December 2022. Along with the aim of reversing type 2 diabetes, he also wanted to reduce weight, improve his quality of life, and minimize medications. Upon enrollment, he underwent a full-body health checkup comprising 72+ parameters, through which it was observed that his creatinine, urine albumin, and serum cholesterol were above the normal range as provided in (Table 1).
| Parameters | Values |
|---|---|
| HbA1c | 12.10% |
| FBS | 186.9 mg/dL |
| Albumin (urine) | 586 mg/L |
| Creatinine | 1.46 mg/dL |
| Total cholesterol | 285 mg/dL |
| Triglycerides | 274 mg/dL |
| LDL | 201.7 mg/dL |
| VLDL | 54.8 mg/dL |
His lifestyle and dietary recall were collected by his personal health coach. Lifestyle was compromised by poor sleep quality, irregular meals, frequent consumption of outside food, and low physical activity. He was also suffering from severe knee pain and exhibited certain symptoms associated with diabetes, such as frequent urination, gastritis, fatigue, increased hunger, blurred vision, and sleeplessness. He also had a family history of type 2 diabetes, with his mother experiencing essential (primary) hypertension. During the time of his enrolment, his vitals, such as weight, height, and BMI, were provided in (Table 2).
| Vitals | Values |
|---|---|
| Weight | 85.3 Kg |
| Height | 174 cm |
| BMI | 28.74 kg/m2 |
He led a sedentary lifestyle with a desk job. His dietary recall included high carbohydrates, high fat, and low protein, with frequent consumption of outside food and a preference for non-vegetarian dishes. Initially, he agreed to reduce consuming excessive amounts of high-fat and high-sugar foods but was unable to adhere to the dietary and exercise interventions. During the program, he was on Glimepiride and Metformin (1-0-1) before meals for lowering blood sugar levels, and Telmisartan 40 mg (0-0-1) for treating high blood pressure.
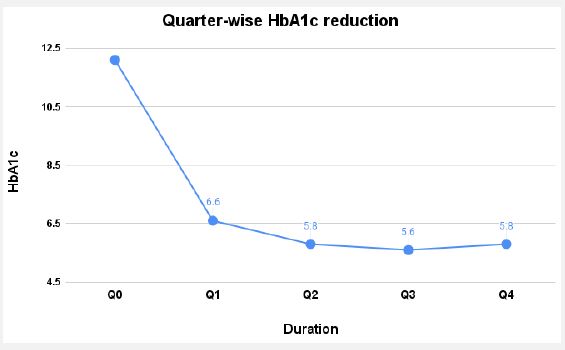
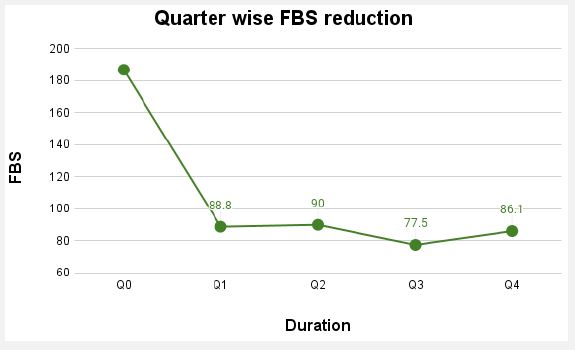
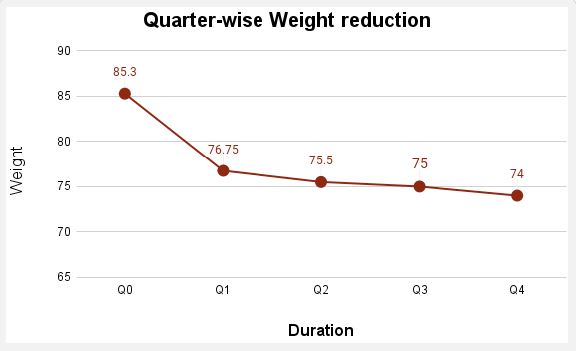
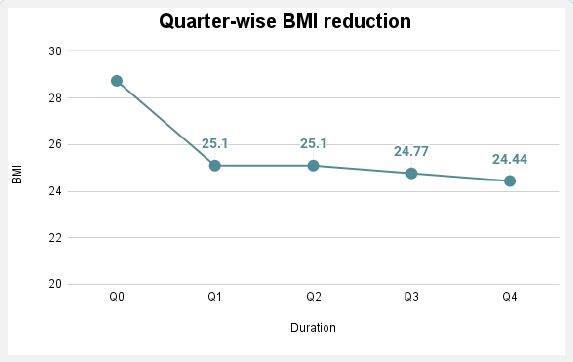
Management and outcome: Mr. CP was assigned a well-experienced doctor and health coach to manage his blood sugar levels and diabetes-related comorbidities. Initially, his health coach assessed his dietary and lifestyle habits to gain a comprehensive understanding of his routine. It was found that Mr. CP was consuming approximately 1800 calories daily. During the initial four days of the CGM period, 64% of blood sugar levels were above the target Time in A Tight Range (TITR) of 80-140 mg/dL, with notable post-meal spikes. To address this, dietary adjustments, and mindfulness and fitness exercises were recommended. These included interventions like chia seeds and fruits for an evening snack, early morning meditation for one-hour, post-meal walks, barley water in the morning, and chamomile tea before bed. These interventions helped lower his blood sugar levels, reducing the proportion of readings above the target range to 27%. Following the dietary adjustments, a structured meal plan was devised in line with the SDRMP recommendations. This plan involved a low-salt and low-protein diet. The total calorie intake was gradually tapered down to 1400 kcal while the protein intake was maintained at 15% along with consumption of up to 40 grams of dietary fibre every day. To address elevated FBS levels and morning lethargy, the pre-breakfast biscuits were swapped with nuts, and the diet was enriched with a variety of nutrient-rich foods, including vegetables, whole grains, lean meats, eggs, lentils, and dairy products. The meal distribution comprised 250-300 kcal for breakfast, 100-150 kcal for mid-morning snacks, 350-400 kcal for lunch, 100-150 kcal for evening snacks, and 300-350 kcal for dinner. Additionally, upon enrolment in the program, he underwent a medication review with his doctor, resulting in adjustments to his prescription, including Linagliptin 5 mg (1-0-0), Metformin 500 mg (1-0-1), and Telmisartan 40 mg (0-0-1). He was gradually introduced to grain-free dinner options, intermittent fasting for 12 hours, and to follow meal sequencing. He was also recommended to make small sachets of salt to keep track of his sodium consumption. Fitness and mindfulness activities were added to his routine, such as a 15-minute walk after both lunch and dinner, and a deep breathing exercise routine before bedtime to improve sleep quality and manage stress. However, he initially found it challenging to adhere to these practices. Gradually, he began incorporating healthier food options and regular exercise into his routine, which led to improved blood sugar levels. Significant reductions were observed in HbA1c, FBS, weight, and BMI. HbA1c levels dropped from 12.1% to 6.6% within 90 days and further decreased to 5.8% by 180 days and sustained till the end of the program (Figure 1). FBS levels decreased from 186.9 mg/dL to 86.1 mg/dL (Figure 2). Additionally, weight was reduced from 85.3 kg to 74 kg, and BMI decreased from 28.74 kg/m² to 24.4 kg/m² (Figure 3).
| Parameters | Values |
|---|---|
| Albumin (urine) | 184.4 mg/L |
| Creatinine | 1.31 mg/dL |
| Total cholesterol | 179 mg/dL |
| Triglycerides | 113.7 mg/dL |
| LDL | 117.2 mg/dL |
| VLDL | 22.7 mg/dL |
In addition to the reduction in blood sugar levels, his medications were also reduced. After the 90-day diagnostic results, he had a consultation with his doctor, during which his medications were changed to Metformin 500 mg (1-0-0) and Telmisartan 40 mg (0-0-1). These doses remained consistent for the next 180 days. He was also prescribed cholecalciferol and mecobalamin supplements to mitigate the risk of deficiencies caused by Metformin. At the end of the program, Metformin was continued, and the dosage of Telmisartan was reduced from 40 mg to 20 mg once a day. He experienced notable improvements in serum cholesterol, creatinine, and urine albumin levels as provided in (Table 3). Additionally, he observed improvements in sleep quality and a reduction in knee pain. He successfully incorporated physical activity and meditation into his daily routine. Alongside losing 10 kg, he also gained muscle strength. His body fat percentage decreased from 26.9% to 24.4%, while his muscle mass increased. His waist circumference was reduced from 96 cm to 84 cm.
In addition to the timely assistance provided by the healthcare professionals, and the progress seen by the client, the quantitative involvement of Mr. CP in the program is noteworthy. During the course of the program, there were 5 doctor consultations, 23 coach consultations, 104 phone calls connected with the coach, over 184 text messages exchanged, and a high adherence to SMBG-self-monitoring of blood glucose with around 240 readings recorded. Data highlights the extensive and multifaceted support provided to Mr. CP.
His impressive path towards better health and glycaemic management reflects his steadfast commitment to the holistic regimen provided by Sugar fit. The pivotal role in achieving favourable results was attributed to his commitment through integration of lifestyle adjustments along with dietary recommendations, as endorsed by the SDRMP. Successful reversal of diabetes is exemplified by the active engagement of clients in their program supported by a dedicated coaching team and general physician consultation. Improvements in HbA1c, FBS levels, and BMI were observed in accordance with effective treatment plans provided by both health coaches and doctors.
Clients receive comprehensive care that addresses both the physiological and lifestyle factors impacting their health through the integration of medical knowledge of a doctor with the practical guidance and support of health coach consultations. It emphasises a holistic approach that considers not only medication but also the importance of daily habits, behaviours, routines and environmental factors in promoting wellness. This integration leads to more effective and sustainable outcomes for diabetic patients in managing their health conditions. Additionally, the study focused on maintaining normal levels of blood pressure, vitamin D3, and vitamin B12 through specific dietary measures along with the use of medications. Later, the dosage of the medication was halved, yet effective diabetes management was still maintained. In conclusion, SDRMP optimises excellent outcomes while minimising potential risks by diligently monitoring the patient’s response and adjusting dosage accordingly. This comprehensive approach to diabetes management effectively monitors and promotes overall health and well-being of people living with diabetes along with a focus on tailoring management strategies to enhance their quality of life.
